
Introduction
You may have noticed that for better or worse we are now in the countdown to a General Election here in the UK, which means the publication of manifestos by all parties, allegedly detailing their key policies and typically providing a glittering away of sweets and toys to win over votes – though in-depth analysis might give an altogether different story, both for what they say and what they fail to mention.
I am renowned for my cynicism of manifestoes and their glossy promises. This brief history of manifesto promises demonstrates amply the fallacy of believing any such pledges, but why in particular? For the questions they fail to answer, for the promises that are substantially changed or quietly forgotten after an election has been won, and for the actions they omit, effectively telling the electorate that this documents mean precisely nothing and form no binding commitment or mandate whatever – all the more since most UK governments achieve a Commons majority with rarely more than 36% of the popular vote.
The prime example of this was the 2012 Health and Social Care Act, no mention of which was made in the Conservative, or for that matter Lib-Dem manifestoes, but was wheeled out as a fully-formed and immense White Paper a few weeks after the election. This is but one example of the cynical politicking that gives Westminster politics a bad name.
A good friend and fellow healthcare devotee Martin Rathfelder asked me to critique Conservative manifesto pledges on healthcare for his Socialist Healthcare Association blog, but as a political neutral (ie. I retain the same dislike and distaste for all political parties, not any one in particular) I think it only right and proper to do an honest comparative critique of Conservative and Labour Manifestos on healthcare and based on my own extensive knowledge and experience, then let readers make up their own mind.
Criteria
Before we start, the framework I shall use in critiquing these policies is as follows:
- That the needs of patients are paramount
- Services must remain free at the point of delivery
- The best thing any party can do is stop meddling in how the NHS is run, to provide resources but stop top-down transformations that have resulted in little benefit but much anguish.
What is not mentioned
These will not be the only omissions, but it’s worth using the examples to demonstrate how unreliable manifestos can be.
- The Conservative manifesto makes no mention whatever of outsourcing contracts for provision of healthcare services previously undertaken by NHS Primary, Community, Acute and Tertiary services, the so-called “privatisation of health”, despite this being a primary feature of the government’s service management within the 2011 Act, and, reputedly, with secret plans to outsource whole Trusts within the next Parliament. This would certainly switch off potential voters loyal to the NHS institutions that have served us for the past 70 years, yet it has not been mentioned in the election campaign.
- The Labour manifesto has dropped entirely a pledge taken in a January statement on healthcare to end all PFI contracts, presumably because somebody realised the cost would amount to £209bn but would offer no immediate benefit to patients but would consume a colossal sum. Labour is promising to invest in capital projects within the NHS but omits to say how much it will commit or on what basis. One could hazard a guess that future projects by a Labour government would not be on the basis of PFI but how they would be funded is not clear.
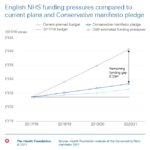
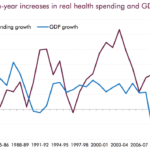
- Budgets: It’s strange but all parties bandy about figures running into multiple billions, yet none make specific commitments to peg NHS spending to a set and higher proportion of GDP, in spite of international aid being pegged at 0.7% of GDP. It’s all smoke and mirrors, of course; HSJ estimates that commitments by both parties would actually reduce NHS spending as a percentage of GDP (see here) and that even in the latest figures we are still a long way below the average proportion (see here) and in 2014 were 6th out of 7 G7 nations in healthcare spending (see here.) Reluctance to do is probably a reflection of the impact on health spending either of a major rise or fall in GDP, bearing in mind the forthcoming Brexit negotiations.





Comparisons
For another view, here is the BBC comparison and here in the Guardian. My considered view follows:
1) The NHS pledge
Labour
In the aftermath of war and national bankruptcy, it was a Labour government that found the resources to create a National Health Service – our proudest achievement, providing universal healthcare for all on the basis of need, free at the point of use. Labour will invest in our NHS, to give patients the modern, well-resourced services they need for the 21st century. Labour will ensure that NHS patients get the world-class quality of care they need and that staff are able to deliver the standards that patients expect.
We will guarantee and uphold the standards of service to which patients are legally entitled under the NHS constitution. By guaranteeing access to treatment within 18 weeks, we will take one million people off NHS waiting lists by the end of the next Parliament.
We will guarantee that patients can be seen in A&E within four hours. By properly resourcing the NHS, Labour will stop the routine breach of safe levels of bed occupancy, and we will end mixed-sex wards. We will deliver the Cancer Strategy for England in full by 2020, helping 2.5 million people living with cancer. And, by properly resourcing ambulance services, we will end the scandal of slowing ambulance-response times.
Conservative
Our National Health Service is the essence of solidarity in our United Kingdom – our commitment to each other, between young and old, those who have and those who do not, and the healthy and the sick. The Conservative Party believes in the founding principles of the NHS. First, that the service should meet the needs of everyone, no matter who they are or where they live. Second, that care should be based on clinical need, not the ability to pay. Third, that care should be free at the point of use. As the NHS enters its eighth decade, the next Conservative government will hold fast to these principles by providing the NHS with the resources it needs and holding it accountable for delivering exceptional care to patients wherever and whenever they need it.
It’s noticeable that both parties are at pains to point out their adherence to the base principles of the NHS, notably that services are “free at the point of delivery” – though how that is maintained and resourced is quite distinct, not that you would necessarily know that from the honeyed words written in their respective manifestos. It will take a brave party to commit to changing those principles, so in all probability when they are changed (and who would bet against it?), it will not appear in any manifesto.
Critics are painting Conservative policy as being the end of the NHS as we know it, with the inevitability of a top-up insurance policy and the option of GP surgeries to levy payments being allowed at some point (bearing in mind we already pay for NHS dental checkups, assuming we can find an NHS dentist willing to include us on their books.)
2) Funding
Labour
Labour will commit to over £30 billion in extra funding over the next Parliament through increasing income tax for the highest 5 per cent of earners and by increasing tax on private medical insurance, and we will free up resources by halving the fees paid to management consultants.
Labour will boost capital funding for the NHS, to ensure that patients are cared for in buildings and using equipment that are fit for the 21st century. And we will introduce a new Office for Budget Responsibility for Health to oversee health spending and scrutinise how it is spent.
Labour will fund free parking in NHS England – for patients, staff and visitors – by increasing the tax on private medical insurance premiums.
Conservatives
…we will increase NHS spending by a minimum of £8 billion in real terms over the next five years, delivering an increase in real funding per head of the population for every year of the parliament….
…we will ensure that the NHS has the buildings and technology it needs to deliver care properly and efficiently. Since its inception, the NHS has been forced to use too many inadequate and antiquated facilities, which are even more unsuitable today. We will put this right and enable more care to be delivered closer to home, by building and upgrading primary care facilities, mental health clinics and hospitals in every part of England. Over the course of the next parliament, this will amount to the most ambitious programme of investment in buildings and technology the NHS has ever seen.
…whilst the NHS will always treat people in an emergency, no matter where they are from, we will recover the cost of medical treatment from people not resident in the UK. We will ensure that new NHS numbers are not issued to patients until their eligibility has been verified. And we will increase the Immigration Health Surcharge, to £600 for migrant workers and £450 for international students, to cover their use of the NHS. This remains competitive compared to the costs of health insurance paid by UK nationals working or studying overseas.
The figures are random and arbitrary, though my experience makes me wary. I recall that the £12bn of new money promised for the NHS in 2011 was swallowed up by the massive cost of implementing the 2012 Health and Social Care Act, though it is true generically that each subsequent government incurs often needless costs by implementing changes that are, for the most part, pointless or hugely damaging. For example, up to the implementation of the 2012 Act 75 % of Acute Trusts were in surplus, but now, and I may be out of date here, something in excess of 80% are in deficit.
During this period the demands of patients has risen steeply, notably emergency admissions, with bed availability at a premium to ensure these patients are treated. There has been no money to bail out Trusts afflicted in this way. Since block contracts (payments assuming a certain number of treatments are performed in a given year) are for the most part replaced by PbR (Payment by Results), in which Acute Trusts are paid only for each patient they treat, but the cost of providing additional resources to provide the additional treatment far outweighs the additional income gained for putting more patients through the system.
There were payments to help Acute Trusts reduce backlogs, but the bureaucracy required by NHSE (and therefore indirectly by the DH) to justify how that money was being spent was formidable, and did not resolve the underlying demand issue.
The real questions both parties have to face are raised daily by the press:
- Is the funding proposed “new money”?
- If so, how is it funded?
Andrew Neil got to the heart of the first question, leaving May looking decidedly shifty:
May was also uncomfortable on the question of whether the £8 billion extra the Tories are proposing for the NHS is all new money or not.
And on the funding question, that was equally vague, all the more ironic since Conservatives have made a point of smearing Labour policies as “tax and spend” – but have not submitted their manifesto pledges to be audited. Whether Labour’s plans stack up in reality remains to be seen, though funding by increasing tax on those earning over £80k and increasing Corporation Tax will satisfy supporters but not the aspirational middle classes or executives – many of whose votes would be essential to win key marginals.
Labour commitment to free parking is superficially attractive but unless policed risks allowing commuters to take advantage of hospital facilities for nothing, at the cost of patients, relatives and staff who need those facilities. The fact is that parking is one of the few non-health related income sources for most Trusts, so any funding commitment requires assurance that the lost income will be made up, quite apart from the costs of maintenance and running parking services. This is not a cheap pledge!
3) STPs, Transformation & Operational Management
Conservative
It is NHS England that determines how best to organise and deliver care in England, set out in its own plan to create a modern NHS – the Five Year Forward View. We support it. We will also back the implementation of the plan at a local level, through the Sustainability and Transformation Plans, providing they are clinically led and locally supported.
We will hold NHS England’s leaders to account for delivering their plan to improve patient care. If the current legislative landscape is either slowing implementation or preventing clear national or local accountability, we will consult and make the necessary legislative changes. This includes the NHS’s own internal market, which can fail to act in the interests of patients and creates costly bureaucracy. So we will review the operation of the internal market and, in time for the start of the 2018 financial year, we will make non-legislative changes to remove barriers to the integration of care.
We expect GPs to come together to provide greater access, more innovative services, share data and offer better facilities, while ensuring care remains personal – particularly for older and more vulnerable people – with named GPs accountable for individual patients. We will support GPs to deliver innovative services that better meet patients’ needs, including phone and on-line consultations and the use of technology to triage people better so they see the right clinician more quickly. We will ensure appropriate funding for GPs to meet rising costs of indemnity in the short term while working with the profession to introduce a sustainable long-term solution.
We will retain the 95 per cent A&E target and the 18-week elective care standard so that those needing care receive it in a timely fashion. We will continue to help the NHS on its journey to being the safest healthcare system in the world.
Labour
Labour will halt and review the NHS ‘Sustainability and Transformation Plans’, which are looking at closing health services across England, and ask local people to participate in the redrawing of plans with a focus on patient need rather than available finances.
The next Labour government will reverse privatisation of our NHS and return our health service into expert public control. Labour will repeal the Health and Social Care Act that puts profits before patients, and make the NHS the preferred provider. We will reinstate the powers of the Secretary of State for Health to have overall responsibility for the NHS.
We will introduce a new legal duty on the Secretary of State and on NHS England to ensure that excess private profits are not made out of the NHS at the expense of patient care. We will invest in our NHS for world-class care
The current changes promoted by the current Conservative government and ongoing are also notable for what is not mentioned as much as what is. For example, the changing priority of resourcing towards urgent and community care means reducing the resourcing for elective care, which in turn means a strong probability that patients requiring hip and knee replacements, to use but one example, may well find themselves waiting years, as in the worst years of the NHS.
The subtext of these plans will be that patients are encouraged to use private healthcare insurance for this kind of procedure, possibly with help from a few carrots in the form of future tax breaks (no manifesto pledge.) Either way, many key targets seem to be on dodgy ground, so inevitably waiting times will rise by weight of pressure on other targets, if the Conservatives have their way.
However. Labour is also promising to re-enforce 18 week national targets and thereby reinforce commitment to elective patients without sacrificing Emergency 4-hour targets, nor indeed Cancer targets – effectively the status quo before STPs came along. For this to work, additional resources at all levels would be essential (see below), but also an effective understanding of where targets distort the delivery of healthcare services by focusing additional resources on areas which are less required in a particular healthcare economy.
The Conservatives also renew their commitment to both, though this rather flies in the face of recent experience where both A&E and 18 week targets have been abandoned, and also in the light of STP strategy where a reduction in commitment to elective surgery is clearly mandated. This paradox was explained by Sir Simon Stevens:
“We are not abandoning the idea that we want very short waits for operations – routine, non-urgent – operations on the NHS,” he said. However, Mr Stevens admitted priority would be placed on A&E, cancer, mental health and GP access before waiting times for “less urgent conditions” were addressed.
He added: “What we’re saying is for the next year, the most important things that the NHS have got to get right and improve on will be A&E services and cancer and mental health and being able to see your family doctor, and we – having got those things right – then want to make sure that we’re also making further progress on our waiting times for less urgent conditions.”
To me this sounds like dancing on the head of a pin, since the effect will almost certainly be an explosion of non-urgent treatment waiting times. You can’t prioritise every service, and electives are always last in line. A sensible government would encourage Trusts to devise achievable local and regional targets based on the local demographic, rather than assuming one size fits all. The flip side of that is the so-called “postcode lottery” whereby services are deemed quicker and/or better in one location rather than another – or the chances of survival improve.
On the face of it, the Conservative manifesto appears to throw responsibility back on to the NHS to manage its own affairs, but this is wholly misleading, as suggested in this well-written analysis. The brief given to Sir Simon Stevens is clear: to save money and reduce patient volumes by any means possible short of charging. However, there is one blinding revelation in this Conservative manifesto, in the form of this statement:
“If the current legislative landscape is either slowing implementation or preventing clear national or local accountability, we will consult and make the necessary legislative changes. This includes the NHS’s own internal market, which can fail to act in the interests of patients and creates costly bureaucracy.”
This implies recognition that their own 2012 Act has been a failure, resulting in gross inefficiency and financial loss – not that they admit the failing was their own! I could have told them that the most important people in any NHS Trust are no longer doctors and nurses but financial controllers and contract managers. The emphasis is entirely wrong and the jury is out on whether the STPs (which, contrary to the government propaganda, have not been chosen by local people, nor even consulted) will make any difference.
After all, closing or merging A&E units is formidably unpopular at any time, and there is little evidence of resources going into community providers to make them work. We know that a substantial branch of community service was outsourced to Virgin without evidence this would be more effective (see here and here. Indeed, Virgin have lost one contract (see here) and are taking the matter to court), but the rumour is that a considerable wedge of NHS services, including the running of hospitals (despite this failure), will be outsourced post-election – of which there is not a word in the manifesto.
Labour’s response is to stop the STP work, though there is little evidence of what they would do instead. However, Labour is promising to “reverse privatisation” – without defining exactly what this means. After all, the NHS is predicated on the services of private GP and dental practices, quite apart from private providers giving essential support to NHS Acute Trusts for flexible capacity – this informal subcontracting was written into the NHS Constitution in 2012.
If they mean by the pledge to reverse contracting out to private providers, that would only happen gradually – and providing the equivalent NHS capacity had not withered in the meantime. The staff are largely the same so the primary difference is whether the management of services is conducted by managers employed directly by the public purse, or those subcontracted to do the job.
Where the Conservatives believe outsourcing to the private sector is more efficient, Labour sees shareholders pocketing millions in dividends from profits earned at the public expense. I suspect never the twain shall agree on this point, though Labour has been pointing out the ministers with shareholdings who benefit from this policy. Putting the responsibility back on the Secretary of State to ensure healthcare standards are delivered may well prove popular.
4) Resourcing
Labour
To guarantee the best possible services for patients, Labour will invest in our health and care workforce. A Labour government will step in with a long-term workforce plan for our health service that gives staff the support they need to do the best for their patients.
Labour will scrap the NHS pay cap, put pay decisions back into the hands of the independent pay review body and give our NHS workers the pay they deserve. Labour will protect patients and legislate to ensure safe staffing levels in the NHS.
Labour’s long-term ambition is for our health system to have the best trained staff in the world, ready to deal with whatever they have to face in the years to come. Labour will re-introduce bursaries and funding for health-related degrees. Labour will support doctors to deliver the best care possible by investing in the training, education and development of doctors throughout their careers.
Labour will immediately guarantee the rights of EU staff working in our health and care services. Labour will support NHS whistleblowers to make sure health service staff are able to speak up in support of the best possible standards for patients. Labour will make it an aggravated criminal offence to attack NHS staff.
Conservative
…we will ensure that the NHS and social care system have the nurses, midwives, doctors, carers and other health professionals that it needs. We will make it a priority in our negotiations with the European Union that the 140,000 staff from EU countries can carry on making their vital contribution to our health and care system. However, we cannot continue to rely on bringing in clinical staff instead of training sufficient numbers ourselves. Last year we announced an increase in the number of students in medical training of 1,500 a year; we will continue this investment, doing something the NHS has never done before, and train the doctors our hospitals and surgeries need.
We will introduce a new GP contract to help develop wider primary care services. We will reform the contract for hospital consultants to reflect the changed nature of hospital care over the past twenty years. We shall support more integrated working, including ensuring community pharmacies can play a stronger role to keep people healthy outside hospital within the wider health system. We will support NHS dentistry to improve coverage and reform contracts so that we pay for better outcomes, particularly for deprived children. And we will legislate to reform and rationalise the current outdated system of professional regulation of healthcare professions, based on the advice of professional regulators, and ensure there is effective registration and regulation of those performing cosmetic interventions.
We will also help the million and more NHS clinicians and support staff develop the skills they need and the NHS requires in the decades ahead. We will encourage the development of new roles and create a diverse set of potential career paths for the NHS workforce. And we will reform medical education, including helping universities and local health systems work closer together to develop the roles and skills needed to serve patients.
We want the NHS to become a better employer. We will strengthen the entitlement to flexible working to help those with caring responsibilities for young children or older relatives. We will introduce new services for employees to give them the support they need, including quicker access to mental health and musculoskeletal services. We will act to reduce bullying rates in the NHS, which are far too high. We will take vigorous and immediate action against those who abuse or attack the people who work for and make our NHS.
The fact is that there is and has been for some considerable time a significant shortage of clinical resources in the NHS at all levels, and attrition rates are at record levels due to poor morale and pay languishing below inflation. It’s not consistent but there is not a Trust in the country that is not having difficulties recruiting experienced senior staff in one specialty or another, especially in rural areas (who cannot offer flexible earning packages to attract more staff), particularly to replace retirees but also many other skilled resources whose dedication has been taken for granted. Not just doctors or nurses either – experienced radiologists, endoscopists, radiographers and other diagnostic technicians, midwives and a host of Associated Healthcare Professional roles are not easy to recruit and have a tendency to leave for career opportunities (see here.)
Yet in the 2015 election we had grand promises spread like confetti on both sides to recruit additional GPs in particular, since that is the front-line resource most stressed. Mr Hunt has been renegotiating GP contracts to ensure they have more money promised in exchange for guaranteeing 7-day working (did anyone ask patients whether they want that?) There is also a model contract for salaried GPs since apparently nobody wants the stress of being a partner in a GP practice any more.
Where would these GPs come from? Since at the time we were not training any more medical students, nor indeed ensuring more stay the demands of their apprenticeship through to specialisation, the answer has to be that more young doctors would be coerced or incentivised to train to be GPs (and trainees are fewer than ever and record numbers do not want to work full-time – see here and here), but at the expense of fewer hospital specialists (from anaesthetists to orthopaedic surgeons, a vast array of essential skills.)
This is why the NHS has been recruiting from abroad at record levels for doctors and specialist nurses – within and beyond the EU. With the Brexit vote the status of these workers has been in some doubt, and a good proportion will undoubtedly leave of their own volition, since the UK is effectively telling them they are not wanted and will have to meet stern criteria to stay, hence the debate about the 140,000 EU workers on which the service depends.
But in practice there will be further shortages we cannot fill without licence to raid the world. The government is peddling additional training places but with nursing bursaries cut and NHS pay frozen there seems little chance they will even staunch the exodus, let alone recruit additional staff. Besides, the shortages are now, not in another 7-10 years when new trainees reach career maturity.
Even if the STPs do reduce the overhead on clinical practitioners (a big ask and far from proven), the Conservative manifesto contains a big black hole on resourcing with a hidden subtext that outsourcing means it’s someone else’s problem and gives the government a convenient scapegoat to blame for not having sufficient staff.
If we were to avoid that fate, Labour’s long-term workforce plan would need to start delivering immediately, which almost certainly means recruiting more experienced staff from overseas. Despite the Commonwealth and the vestiges of a colonial past, bringing people from overseas is not a long-term solution since they are rightly needed in their own countries and typically come here, ironically, because earnings are higher. One suspects the differentials are being eroded daily.
But final word on this topic must be devoted to the NHS pay cap, which the Conservatives are pledged to continue. There seems little doubt that NHS resources will continue to bleed away, not just to other options within health but also to other professions entirely since they can earn more elsewhere. If each 1% pay rise for NHS staff costs £500m, funding must be clear, but the impact of not paying staff more could easily prove disastrous, especially after an 11% rise for MPs.
Apart from the actual money it tells staff they are not valued, and their dedication and commitment to the service, despite being underpaid and overworked, has been taken for granted. The Junior Doctors strikes over their contracts, but it is not beyond the realms of possibility that a wider strike over pay may follow, and not as a gesture of defiance from hard left union leaders either; morale in the NHS is dangerously low and is close to breaking point. Any government would ignore the signs at their peril.
5) Mental Health
Conservative
It was Conservatives in government that gave parity of esteem to the treatment of mental health in the National Health Service. We have backed this with a significant increase in 57 funding: since 2010 we have increased spending on mental health each year to a record £11.4 billion in 2016/17, with a further investment of £1 billion by 20/21, so that we can deliver the mental health services people deserve. We will now build on this commitment.
First, we will address the need for better treatments across the whole spectrum of mental health conditions. We will make the UK the leading research and technology economy in the world for mental health, bringing together public, private and charitable investment.
Improving treatment services will not be sufficient, however. We will also reform outdated laws to ensure that those with mental illness are treated fairly and employers fulfil their responsibilities effectively.
The current Mental Health Act does not operate as it should: if you are put on a community treatment order it is very difficult to be discharged; sectioning is too often used to detain rather than treat; families’ information about their loved ones is severely curtailed – parents can be the last to learn that their son or daughter has been sectioned. So we will introduce the first new Mental Health Bill for thirty-five years, putting parity of esteem at the heart of treatment.
We will transform how mental health is regarded in the workplace. We will amend health and safety regulations so that employers provide appropriate first aid training and needsassessment for mental health, as they currently do for risks to physical health, and extend Equalities Act protections against discrimination to mental health conditions that are episodic and fluctuating. We will consider the findings of the Stevenson-Farmer Review into workplace mental health support, working with employers to encourage new products and incentives to improve the mental health and wellbeing support available to their employees. And, as we did with Dementia Friends, we will train one million members of the public in basic mental health awareness and first aid to break the stigma of mental illness.
We understand the massively increased pressures on young people’s mental health. We will take focused action to provide the support needed by children and young people. Half of all mental health conditions become established in people before the age of fourteen. So we will ensure better access to care for children and young people. A Conservative government will publish a green paper on young people’s mental health before the end of this year. We will introduce mental health first aid training for teachers in every primary and secondary school by the end of the parliament and ensure that every school has a 73 single point of contact with mental health services. Every child will learn about mental wellbeing and the mental health risks of internet harms in the curriculum. And we will reform Child and Adolescent Mental Health Services so that children with serious conditions are seen within an appropriate timeframe and no child has to leave their local area and their family to receive normal treatment.
Labour
Mental ill-health is the biggest unaddressed health challenge of our age. Around one in four people in the UK will experience a mental health problem each year.
Yet, since 2010 mental health funding has been cut, the number of mental health nurses has fallen by 6,600 and remaining mental health budgets have been raided to plug holes elsewhere in the NHS.
Labour will work to reverse the damage done to mental health services under this Tory government, which is particularly hitting services for LGBT and BAME communities.
In order to protect services, we will ring-fence mental health budgets and ensure funding reaches the frontline.
We will end the scandal of children being treated on adult mental health wards and stop people being sent across the country, away from their support networks, to secure the treatment they need by bringing forward the ending of out-of-area placements to 2019.
Labour will also bring an end to the neglect of children’s mental health. Half of people with mental health problems as adults present with symptoms by the age of 14. Yet, across England only 8 per cent of mental health funding goes to services for children and young people. In recent years, referrals to Child and Adolescent Mental Health Services have increased by two-thirds, and the number of young people presenting to A&E units with psychiatric conditions has doubled. Suicide is now the most common cause of death for boys aged between five and 19.
Labour will invest in early intervention by increasing the proportion of mental health budgets spent on support for children and young people. We will ensure that access to a counselling service is available for all children in secondary schools.
Giving mental health the same priority as physical health means not only ensuring access to services, but also making improvements, to those services. Choice is important in a modern NHS, and patients who receive their therapy of choice have better outcomes. Labour will therefore ask the National Institute for Health and Care Excellence (NICE) to evaluate the potential for increasing the range of evidence- based psychological therapies on offer.
Labour will focus resources on services to provide care closer to home and deliver a truly 21st century health system. We will work towards a new model of community care that takes into account not only primary care but also social care and mental health. We will increase funding to GP services to ensure patients can access the care they need. And we will halt pharmacy cuts and review provision to ensure all patients have access to pharmacy services, particularly in deprived or remote communities.
Labour will tackle the growing problem of rationing of services and medicines across England, taking action to address ‘postcode lotteries’ and making sure that the quality of care you receive does not depend on which part of the country you live in. We will ensure all NHS patients get fast access to the most effective new drugs and treatments, and insist on value-for-money agreements with pharmaceutical companies.
To make sure that autistic people are able to access the whole of their community and to put an end to social isolation, Labour will set the ambition to make our country autism-friendly. We will ensure that everyone with a long-term condition, such as those with diabetes, will have the right to a specialised care plan, and access to condition-management education. We will ensure highquality, personalised care for people approaching the end of their life, wherever and whenever they need it.
Labour will ensure that NHS England completes the trial programme to provide PrEP (pre-exposure prophylaxis) as quickly as possible, and fully roll out the treatment to high-risk groups to help reduce HIV infection.
Famously described as the “Cinderella service”, mental health is a prime example of the paradox and hypocrisy of government. They will tell you they have ploughed in £Xm extra for the treatment of mental health yet everyone at ground level will tell you there have been consistent and swingeing cuts over many years. It’s like supermarkets blazing TV adverts to tell you they have cut 20p off one product but ignoring the price rises on a hundred more.
The past commitments include the pledge that mental health would be that they are treated with equivalence to physical ailments, yet the reality is that acute and chronic patients can rarely get appropriate treatments within their own areas. Cut off from family and friends, people put in this position are likely to get worse before they get better, yet neither party is committing to guaranteed local treatments, even if Labour is talking about providing services via secondary schools and Conservatives into workplace support – both of which I will believe when I see them operating nationally.
There was a time when access to mental health treatments was to be covered by the same 18 week target applied to elective physical treatments, until it was realised that this is not remotely achievable or meaningful – no mention in either manifesto there. Money, even if it were true, is not a substitute for achievement, and there is a massive performance gap on all mental health services, and as Labour rightly points out MH budgets have been raided to cope with crises elsewhere.
It is almost as bad as the Victorian asylum strategy and certainly far from the original community treatment strategy gradually devised and instituted from the 70s on, and all the worse for the fact that getting discharges is as difficult as getting treatments.
But it isn’t merely severe cases that suffer. Taking mild depression as one example, the government has talked up (no pun intended) the need for talking therapies, especially CBT, rather than giving out antidepressants like sweeties – but has not provided the resource for a sustained and consistent national approach to delivering CBT. Even then, I would be very wary of assumptions that any one approach can be a panacea.
For the Conservative manifesto, the question it begs is why they have not done these things in the past 7 years of power, since they were equally wanting in 2010. Equally, why budgets were slashed then money allegedly thrown at the problem.
As with all other forms of care, the resource shortage will not be refilled overnight, any more than other commitments will be delivered instantly. In this case, I doubt either set of pledges will survive long in the heat of government priorities. The Cinderella Service will be put on the back burner once again.
6) Social Care
Conservatives
We will build on the proud Conservative record in supporting those with disabilities, including the landmark Disability Discrimination Act of 1995. We want to see attitudes to disability shift as they have for race, gender and sexuality in recent years: it should be completely unacceptable for people with disabilities to be treated negatively.
We will get 1 million more people with disabilities into employment over the next ten years. We will harness the opportunities of flexible working and the digital economy to generate jobs for those whose disabilities make traditional work difficult. We will give employers the advice and support they need to hire and retain disabled people and those with health conditions. We will continue to ensure a sustainable welfare system, with help targeted at those who need it most. We will legislate to give unemployed disabled claimants or those with a health condition personalised and tailored employment support.
We believe that where you live, shop, go out, travel or park your car should not be determined by your disability. So we will review disabled people’s access and amend regulations if necessary to improve disabled access to licensed premises, parking and housing. We will work with providers of everyday essential services, like energy and telecoms, to reduce the extra costs that disability can incur.
Our system of care for the elderly is not working for the hundreds of thousands currently not getting the dignified and careful attention they deserve, nor for the people and organisations providing that care, nor is it sustainable for today’s younger people who will potentially one day face care costs themselves. It is not fair that the quality of care you receive and how much you pay for it depends in large part on where you live and whether you own your own home. Where others have failed to lead, we will act. We have already taken immediate action, putting £2 billion into the social care system and allowing councils to raise more money for care themselves from Council Tax. We are now proposing medium and long-term solutions to put elderly care in our country on a strong and stable footing.
Under the current system, care costs deplete an individual’s assets, including in some cases the family home, down to £23,250 or even less. These costs can be catastrophic for those with modest or medium wealth. One purpose of long-term saving is to cover needs in old age; those who can should rightly contribute to their care from savings and accumulated wealth, rather than expecting current and future taxpayers to carry the cost on their behalf. Moreover, many older people have built considerable property assets due to rising property prices. Reconciling these competing pressures fairly and in a sustainable way has challenged many governments of the past. We intend to tackle this with three connected measures.
First, we will align the future basis for means-testing for domiciliary care with that for residential care, so that people are looked after in the place that is best for them. This will mean that the value of the family home will be taken into account along with other assets and income, whether care is provided at home, or in a residential or nursing care home.
Second, to ensure this is fair, we will introduce a single capital floor, set at £100,000, more than four times the current means test threshold. This will ensure that, no matter how large the cost of care turns out to be, people will always retain at least £100,000 of their savings and assets, including value in the family home.
Third, we will extend the current freedom to defer payments for residential care to those receiving care at home, so no-one will have to sell their home in their lifetime to pay for care.
We believe this powerful combination maximises protection for pensioner households with modest assets, often invested in the family home, while remaining affordable for taxpayers. We consider it more equitable, within and across the generations, than the proposals following the Dilnot Report, which mostly benefited a small number of wealthier people.
An efficient elderly care system which provides dignity is not merely a function of money. So our forthcoming green paper will also address system-wide issues to improve the quality of care and reduce variation in practice. This will ensure the care system works better with the NHS to reduce unnecessary and unhealthy hospital stays and delayed transfers of care, and provide better quality assurance within the care sector. We will reduce loneliness and promote technological solutions to prolong independent living, and invest in dementia research. As the majority of care is informally provided, mainly by families, we will give workers a new statutory entitlement to carer’s leave, as enjoyed in other countries.
Creating a sustainable elderly care system means making decisions about how the rising budget devoted to pensioners is spent, so we will target help where it is needed most. So we will look at Winter Fuel Payments, the largest benefit paid to pensioners, in this context. The benefit is paid regardless of need, giving money to wealthier pensioners when working people on lower incomes do not get similar support. So we will meanstest Winter Fuel Payments, focusing assistance on the least well-off pensioners, who are most at risk of fuel poverty. The money released will be transferred directly to health and social care, helping to provide dignity and care to the most vulnerable pensioners and reassurance to their families. We will maintain all other pensioner benefits, including free bus passes, eye tests, prescriptions and TV licences, for the duration of this parliament.
Labour
Our social care sector is in crisis, with severe consequences for the quality of care, public finances, personal assets, pressures on unpaid carers of family and friends, and delays to discharging patients from hospitals.
Care services have been slowly but relentlessly privatised. In recent years, one in ten people reaching the age of 65 have faced lifetime care costs of over £100,000, with some homeowners paying the entire value of their homes.
The Conservatives’ cuts have led to £4.6 billion lost from social care budgets, despite rising demand. Around 1.2 million older people have care needs that are going unmet. Care in the community has become a cover for unseen neglect.
In our first term, Labour will lay the foundations of a National Care Service for England.
Our first urgent task will be to address the immediate funding crisis. We will increase the social care budgets by a further £8 billion over the lifetime of the next Parliament, including an additional £1 billion for the first year. This will be enough for providers to pay a real living wage without cutting the quality of care they provide. It will allow implementation of the principles of the Ethical Care Charter, already adopted in 28 council areas, ending 15-minute care visits and providing care workers with paid travel time, access to training and an option to choose regular hours.
Labour will also increase the Carer’s Allowance for unpaid full-time carers to align the benefit with rates of the Jobseeker’s Allowance.
Short-term funding solutions will not address the fundamental long-term challenges of our ageing demographics, nor meet the growing demands arising from late-life illnesses.
The National Care Service will be built alongside the NHS, with a shared requirement for single commissioning, partnership arrangements, pooled budgets and joint working arrangements. We will build capacity to move quickly towards a joined-up service that will signpost users to all the appropriate services at the gateway through which they arrive.
In its first years, our service will require an additional £3 billion of public funds every year, enough to place a maximum limit on lifetime personal contributions to care costs, raise the asset threshold below which people are entitled to state support, and provide free end of life care. There are different ways the necessary monies can be raised. We will seek consensus on a cross-party basis about how it should be funded, with options including wealth taxes, an employer care contribution or a new social care levy.
Improving the quality of social care is a vital part of providing dignity in older age and independence and support for people who are vulnerable or have a disability or a mental health condition.
Labour will build a new National Care Service. We will also set out the funding alternatives clearly and honestly, seeking to implement change through consensus. Providing dignity and care in old age should transcend party politics and campaign slogans.
It’s almost as if the shortfall in social care comes as a surprise to politicians every few years. Bed blocking through delayed transfers of care from hospital is not a new problem, and has been steadily getting worse as the volume of admissions rise. But then the lack of an effective integrated strategy has always been a problem since the decision was taken to make social care the responsibility of local authorities and not combine it within NHS service provision back in the 40s, but the position has been much exacerbated by the cutting of LA budgets to the bone, the gradual erosion of Local Authority-owned care homes and nursing homes, and the fact that the private homes are also in decline since there is little profit at rates paid by the LAs.
Time was when people in their dotage were cared for by extended families, though that is seldom an option nowadays, since couples with children live in boxy houses on estates, both partners work and money to pay out on day-to-day home help for independent oldies is expensive, without the vast burden of round-the-clock residential nursing care for those who lose the lottery and suffer neurologically or physically degenerative conditions lasting years.
Keeping people independent is a worthwhile objective, but as Labour rightly points out, “care in the community has become a cover for unseen neglect.” The rates paid to carers have come under scrutiny in recent years, but in manifestos the discussion is on the big sums rather than the people who drudge at below minimum wage. Labour commitments to end the 15-minute care visit, to be paid for travel time and to ensure those employed on zero hour contracts get the option of standard hours and benefits are welcome, though there is still a great shortage of carers – the most valuable yet least rewarded people in our society.
The real factor under discussion is the impact of means-testing: how much will people have to pay from their estate and how much they will can keep to give in inheritance tax to pass on, assuming they choose not to fund care privately? The catch is that for the promise nobody’s home will have to be sold to fund care (once the biggest bugbear for the middle classes), it will be paid retrospectively.
The Conservatives, a party instinctively committed to the abolition of inheritance tax, got their fingers burned through this statement, labelled “dementia tax” by the press, and which seemed to take them wholly by surprise:
…to ensure this is fair, we will introduce a single capital floor, set at £100,000, more than four times the current means test threshold. This will ensure that, no matter how large the cost of care turns out to be, people will always retain at least £100,000 of their savings and assets, including value in the family home.
Tory supporters were up in arms, not least in her very affluent Maidenhead constituency, where house owners would have most to lose – in short, the commitment to fund was limitless. Hence what appeared to be a u-turn by Mrs May to state that care payments would be capped. The question then becomes how Mrs May would fund what appears to be a potentially vast and almost open-ended commitment for care LA’s could not afford.
Unfortunately, while means testing affects those whose wealth may be impacted directly. the real sufferers are those who cannot afford to pay and therefore have to take what they are given, based on LA resourcing. Carers get an allowance, but the erosion of DLA and other benefits make it harder to gain the support needed to live a normal life, quite apart from the issues affecting the elderly. The default will be for families to help where services are not readily provided in the short term.
It’s not very clear how effective the Labour pledges could be since there is insufficient detail to judge them by, though the key differences appear to be no mention of means testing and better integration with the NHS for the long-term management of degenerative illnesses. Perhaps a full integration package could have been included?
7) Quality of Care & Outcomes
Labour
We will create a new quality, safety and excellence regulator – to be called ‘NHS Excellence’.
Conservative
..we will implement the recommendations of the Accelerated Access Review to make sure that patients get new drugs and treatments faster while the NHS gets best value for money and remains at the forefront of innovation.
Outcomes in the NHS for most major conditions are considerably better than three, five or ten years ago. However, the founding intention for the NHS was to provide good levels of care to everyone, wherever they live. This has not yet been achieved: there remain significant variations in outcomes and quality across services and across the country. We will act to put this right.
To help the NHS provide exceptional care in all parts of England, we will make clinical outcomes more transparent so that clinicians and frontline staff can learn more easily from the best units and practices, and where there is clear evidence of poor patient outcomes, we will take rapid corrective action. We will ensure patients have the information they need to understand local services and hold them to account.
We will empower patients, giving them a greater role in their own treatment and use technology to put care at their convenience. In addition to the digital tools patients already have, we will give patients, via digital means or over the phone, the ability to book appointments, contact the 111 service, order repeat prescriptions, and access and update aspects of their care records, as well as control how their personal data is used. We will continue to expand the number of NHS approved apps that can help monitor care and provide support for physical and mental health conditions. We will pilot the live publication of waiting times data for A&Es and other urgent care services. We will further expand the use of personal budgets. We will also continue to take action to reduce obesity and support our National Diabetes Prevention Programme.
Our ambition is also to provide exceptional care to patients whenever they need it. That is why we want England to be the first nation in the world to provide a truly seven-day healthcare service. That ambition starts with primary care. Already 17 million people can get routine weekend or evening appointments at either their own GP surgery or one nearby, and this will expand to the whole population by 2019.
In hospitals, we will make sure patients receive proper consultant supervision every day of the week with weekend access to the key diagnostic tests needed to support urgent care. We will also ensure hospitals can discharge emergency admissions at a similar rate at weekends as on weekdays, so that when someone is medically fit to leave hospital they can, whichever day of the week it is.
We will extend the scope of the CQC to cover the health-related services commissioned by local authorities. We will legislate for an independent healthcare safety investigations body in the NHS. We will require the NHS to continue to reduce infant and maternal deaths, which remain too high.
Labour has relatively little to say on quality of care and outcomes, possibly the greatest strength of Conservative pledges, other than set up yet another new regulator and engage in consultation on what plans are required. Why there would be a need for yet another body to provide monitoring and regulation is not clear, but if the CQC is not already there to measure and ensure excellence, what is it there to do?
However, Labour does pledge commitment and funding to provide a “world class NHS” – though the definition of “world class” is less than clear.
Of the Conservative pledges, 7-day service seems the least credible since the service already operates round the clock in every hospital and provides out of hours services and 111 as options to enable help for those who need it – quite apart from A&E. In hospitals the use of Junior Doctor and Consultant Contracts is a vehicle to bring about 7-day shifts without paying any more for the privilege. It will demonstrate that there are insufficient resources to fill shifts.
The impact on non-urgent community based provision 7 days is less clear, quite apart from the reluctance of already stressed GPs to continue adding to their already impossible work load. Walk-in centres provide one form of non-urgent service, usually on Saturday mornings too, but it is less than clear what demand there is for these services on Sunday evenings, for example.
8) Public Health, Children’s Care etc.
Labour
For our health and care services to be sustainable in the long term, we need a renewed commitment to keeping people fit and well. Labour will focus our efforts on children’s health, protecting the wellbeing of the nation for the decades to come.
We will take action to significantly reduce infant deaths and to ensure all families who lose a baby receive appropriate bereavement support.
Labour will invest in children’s health, bringing in a new government ambition for our children to be the healthiest in the world. We will fight health inequalities to break the scandalous link between child ill-health and poverty. We will introduce a new Index of Child Health to measure progress against international standards, and report annually against four key indicators: obesity, dental health, under-fives and mental health. We will set up a new £250 million Children’s Health Fund to support our ambitions. As part of a preventative healthcare drive, Labour will increase the number of health visitors and school nurses
We will publish a new childhood obesity strategy within the first 100 days, with proposals on advertising and food labelling. We will make a concerted effort to address poor childhood oral health in England. Labour will implement the Soft Drinks Industry Levy, commonly known as the ‘sugar tax’.
We will implement a strategy for the children of alcoholics based on recommendations drawn up by independent experts.
Labour will implement a Tobacco Control Plan, focusing on issues of mental health and young smokers.
Loneliness is an increasing problem for our society, and as Jo Cox put it, “young or old, loneliness doesn’t discriminate”. A Labour government will create a more equal society for the many by working with communities, civil society and business to reduce loneliness.
Labour will address historic public- health injustices. We will hold a public enquiry into contaminated blood. We will also hold a public inquiry into medicines, including Valproate, medical devices and medical products licensing and regulation.
A Labour government would maintain our commitment to improve sexual-health services, especially HIV services which will include reducing the rates of undiagnosed and late- diagnosed HIV, ending the stigma of HIV in society, and promoting the increased availability of testing and treatment.
Our commitment to consistent high quality care for everyone applies to all conditions. We will set new standards in some priority areas and also improve our response to historically underfunded and poorly understood disease groups.
In cancer services, we will deliver the new promise to give patients a definitive diagnosis within 28 days by 2020, while expanded screening and a major radiotherapy equipment upgrade will help ensure many more people survive cancer.
We will continue to rectify the injustice suffered by those with mental health problems, by ensuring that they get the care and support they deserve. So we will make sure there is more support in every part of the country by recruiting up to 10,000 more mental health professionals. We shall require all our medical staff to have a deeper understanding of mental health and all trainees will get a chance to experience working in mental health disciplines; we shall ensure medical exams better reflect the importance of this area. And we will improve the co-ordination of mental health services with other local services, including police forces and drug and alcohol rehabilitation services.
We have a specific task to improve standards of care for those with learning disabilities and autism. We will work to reduce stigma and discrimination and implement in full the Transforming Care Programme.
We will improve the care we give people at the end of life. We will fulfil the commitment we made that every person should receive attentive, high quality, compassionate care, so that their pain is eased, their spiritual needs met and their wishes for their closing weeks, days and hours respected. We will ensure all families who lose a baby are given the bereavement support they need, including a new entitlement to child bereavement leave.
We believe government has a role to play in helping young people get the best possible start in life. We are seeing progress: smoking rates are now lower than France or Germany, drinking rates have fallen below the European average and teenage pregnancies are at record lows. We will continue to take action to reduce childhood obesity. We will promote efforts to reduce unhealthy ingredients and provide clearer food information for consumers, as our decision to leave the European Union will give us greater flexibility over the presentation of information on packaged food. We shall continue to support school sport, delivering on our commitment to double support for sports in primary schools.
The greater emphasis on public health in both manifestos is notable as the best available way to prevent the need for treatment of our costliest conditions (heart disease, diabetes, cancers etc.), but it has a long way to go yet.
For example, no government campaign yet has had a significant impact on childhood obesity – or any other form of obesity come to that. If they were offering free gym memberships and giving out free vegetables, I doubt there would be that many takers. This is a complex societal issue that cannot easily be solved. A sugar tax or pressure applied on manufacturers to reduced refined sugar in products is merely one tentative step in the right direction.
After all, smoking took decades to reduce, helped by strong legislation to prevent smoking in public places. It will take similarly tough measures to control drinking as well as obesity, though I doubt either Conservatives or Labour has the will to take really tough decisions here.
If Public Health is the future, it will need more thought, considerably more investment, and also much greater courage from governments about confronting the issues head on and not giving way to lobby groups from the businesses impacted. Frankly I have little faith there is true courage in government, since self-preservation and taking the path of least resistance usually comes out on top.
Conclusion
While there is no doubt much thought and at least some detail has gone into these manifestos, my conclusion is that they do not answer the questions, they omit many key pieces of information, they imply much more radical approaches and the fail to mention how critical planks of policy will be achieved. If I had my way there would be a legal obligation on parties to disclose all plans, and to deliver everything promised in manifestos, though I realise it will never happen.
As for healthcare, I can’t see any party helping to save a great service from the mess they have got it into – at least not within the next parliament, and not within the current strategy planned by Simon Stevens. I suspect if I were writing this blog in another 20 years the landscape might be radically different, though not in the way documented by manifesto commitments.