23 Feb 2014
This is yet another blog about healthcare issues, along with genetic predisposition, the effects of ageing and more besides.
Yes, medical science has improved and yes, we are are living longer, but there is a creeping dependency on interventions from the medical professions, in which running repairs will increase in frequency. Since we all unavoidably die of some cause at some time, there’s a degree of inevitability that some things will go wrong with the body that carried you thus far, so chances are that whatever happened previously we will live the second half of our lives dealing with ailments giving us varying levels of inconvenience and discomfort.
Granted there are plenty who claim they are fit as the proverbial until the day they drop dead of heart disease, but most of us will find the ills of ageing afflict us gradually over a period of years. I’m 54 and, being far from a hypochondriac, feel generally lucky that my health has kept me in good fettle up to the past year or so. Since then it’s been one thing after another, largely one-off transactional problems (since you can only dispose of your appendix once without the fear it might grow back to haunt you, for example), and of the range of permanent chronic afflictions I could do far worse in the scheme of things than be slightly hard of hearing; that and short-term memory loss that some might diagnose as early-onset Alzheimers but I consider to be a touch of eccentric memory loss.
However, there was always a ticking time bomb in the form of genes, until such times as genetic engineering has found a way to iron out our deficiencies and predispositions long before they ever start to inhabit our bodies (this inspires visions of scenes from The Exorcist, though you would be pretty unlucky to inherit head-spinning.)







In my case, the one I always knew would catch up sooner or later was type 2 diabetes. My paternal grandmother injected herself with sufficient insulin to kill a horse for 60-odd years, until such time as a doctor actually looked at the prescription and decided the prospects of a legal challenge should best be avoided, and therefore stopped the dose. It was a memory from childhood that always made me shudder, but the inevitability was brought home when my dad was also diagnosed diabetic. Never a small chap and always fond of his food, his exercise levels dropped off after his beloved golden retriever, Benjie, died in 1992. Dad got his medication in oral form, but I don’t recall him changing his lifestyle any, other than through rheumatoid arthritis that racked him with pain.
Before going on, probably a good idea to give a little background for the uninitiated, and let’s face it, most of us non-obsessives would sooner not know more than we need to about medical conditions. But here we go:
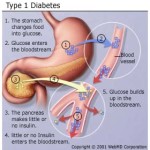
Diabetes mellitus type 2 (formerly noninsulin-dependent diabetes mellitus (NIDDM) or adult-onset diabetes) is a metabolic disorder that is characterized by high blood sugar in the context of insulin resistance and relative lack of insulin. This is in contrast to diabetes mellitus type 1, in which there is an absolute lack of insulin due to breakdown of islet cells in the pancreas. Type 2 diabetes makes up about 90% of cases of diabetes, with the other 10% due primarily to diabetes mellitus type 1 and gestational diabetes. Obesity is thought to be the primary cause of type 2 diabetes in people who are genetically predisposed to the disease.
Type 2 diabetes is initially managed by increasing exercise and dietary changes. If blood sugar levels are not adequately lowered by these measures, medications such as metformin or insulin may be needed. In those on insulin, there is typically the requirement to routinely check blood sugar levels.
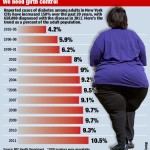
Rates of type 2 diabetes have increased markedly since 1960 in parallel with obesity. As of 2010 there were approximately 285 million people diagnosed with the disease compared to around 30 million in 1985. Long-term complications from high blood sugar can include heart disease, strokes, diabetic retinopathy where eyesight is affected, kidney failure which may require dialysis, and poor blood flow in the limbs leading to amputations.
So I’ve been expecting it for some years but always tested negative before. That said, friends noticed long before I that I have a tendency towards fatigue, and when I feel tired I seem to have an unquenchable thirst. And for that matter I’ve been peeing for England of late. Blow me, when it was suggested to me I looked up the symptoms and look what I found:
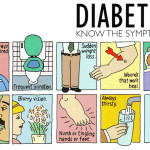
The classic symptoms of diabetes are polyuria (frequent urination), polydipsia (increased thirst), polyphagia (increased hunger), and weight loss. Other symptoms that are commonly present at diagnosis include a history of blurred vision, itchiness, recurrent vaginal infections, and fatigue. Many people, however, have no symptoms during the first few years and are diagnosed on routine testing.
OK, no vaginal infections since I’m not suitably equipped, nor any noticeable weight loss or blurred vision, but polyuria, polydipsia and fatigue are cast iron certainties. Must also admit to having being a tad itchy and nibblish too, though as soon as I read that I was scratching my head en route to making a small sandwich.
Nonetheless, sufficient to get tested, but being reluctant to book GP appointments at a time of unprecedented demand without some good reason, I chose to tuck away the blood sugar test as a secondary during an appointment about a minor ailment, namely tennis elbow. I mentioned it in passing: can I book a blood test for diabetes, given my family history?
The GP was less laid back about it. He listened to me, asked questions, then took out a little digital device for measuring blood sugar, pricked my finger, fed it into the machine, then up popped the read-out: 16.3. Being a layman, I had no idea whether the norm was 1, 10, 100 or 1,000, though he assured me that (a) my blood sugar reading should be around 7, and (b) that mine was sufficiently high, even allowing for an error margin, to take immediate action. So the GP filled out a form and told me to get myself hence to Colchester on Monday morning for a blood test, and to expect a call from the diabetic nurse later in the day. That is, by the standards of general practice, pretty rapid action.
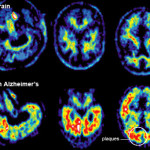
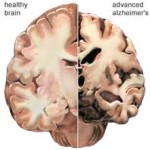
Hit pause button a second. A minor detour on other inherited conditions while I think about it. Remember the grandmother I mentioned above in the context of diabetes? The very same grandmother developed Alzheimers late in life, which may or may not make me prone, if I live long enough.
Another concern is rather closer to hand: my dad had prostate cancer, among other ailments. There is rumoured to be an increased susceptibility if you have a family history. I’ll almost certainly be clear, though there is a possibility I may get diagnosed at some point in the future, since prostate cancer often presents no symptoms for a considerable time even when you are positive, though the upside is that masturbation helps to prevent it (allegedly.) But no matter what your nocturnal habits, guys, the quacks apparently recommend that when you get to my age an annual PSA test is desirable if you have family history.
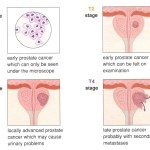
Stage one is generally inexact science in the form of the middle aged GP pulling on latex gloves to stick a finger in your bottom, which fumbling works only if you have a hugely enlarged prostate, in which case you would probably have many problems peeing. The very thought of such a humiliation sets the vast majority of straight men into a frenzy of anxious buttock-clenching, but is in fact nothing like the terrible ordeal feared. However, the blood test is desirable. Its downside is a tendency towards false positive readings, which, erring on the side of caution, is probably better than false negatives. More background:
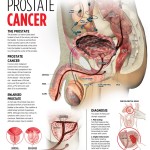
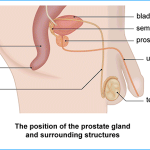
Prostate cancer is a form of cancer that develops in the prostate, a gland in the male reproductive system. Most prostate cancers are slow growing; however, there are cases of aggressive prostate cancers. The cancer cells may metastasize (spread) from the prostate to other parts of the body, particularly the bones and lymph nodes. Prostate cancer may cause pain, difficulty in urinating, problems during sexual intercourse, erectile dysfunction, or death. Other symptoms can potentially develop during later stages of the disease.
Rates of detection of prostate cancers vary widely across the world, with South and East Asia detecting less frequently than in Europe, and especially the United States. Prostate cancer tends to develop in men over the age of fifty. Globally it is the sixth leading cause of cancer-related death in men (it is now the first in the UK and second in the United States). Prostate cancer is most common in the developed world with increasing rates in the developing world. However, many men with prostate cancer never have symptoms, undergo no therapy, and eventually die of other unrelated causes. Many factors, including genetics and diet, have been implicated in the development of prostate cancer. Recently the prevalence of light pollution has been implicated in the development of prostate cancer.
Now women are more in control of their specific testing, diagnostic and treatment pathways, it’s nice to see that men are being invited to do the same in the UK, courtesy of the advertising campaign starring Bill Bailey (see here and here.)
So…. back to my GP’s surgery. I casually dropped this background into the conversation with the doc after hearing his proposed course of action: if you are ordering a blood test, can you order the PSA test at the same time. Yes, I know about the false positives, but it’s been a couple of years and…. Even as I spoke he was ticking the boxes on the form, leaving me contemplating the distinct possibility that I might end up on Monday with at least two positives and the prospect of being medicated twice over.
Strange as it might sound, and contrary to the fears of friends, this does not especially worry me, not even “the big C”. If anything, I’m far more worried about dealing with our friends at HMRC and the DVLA. With a keen sense of fatalism and, as mentioned, the inevitability that my demise will occur by one means or another, I’m pretty chilled about it all and not squeamish. If I’m in extreme pain that may change, but then again I coped moderately well with kidney stones and a gangrenous appendix, so chances are that I have a moderately high pain threshold. Better hone my gallows humour for that eventuality, but in the meantime just go through whatever treatment follows with the same sense of humour.
Enough with the bravado. Bear in mind I’m not really suffering at all right now, so the issue you have to deal with is the future threat: complications of diabetes can shorten life by up to 10 years, and prostate cancer, untreated, can be fatal. The thing about diabetes is that managing it is as much about exercise and diet as medication, maybe more so. Slight lifestyle retraining and monitoring required, possibly a reduction in the special treats one allows myself, but nothing too radical considering the condition is incurable. The point is that something will go wrong at some point so be prepared.
Against that, the treatment path for the worst cases of cancer can be almost as nasty as the disease. I’ve known female friends treated for breast cancer undergoing 6 or 8 rounds of chemo followed by radiotherapy, which poisons you would sooner avoid if at all possible. My dad‘s prostate cancer was caught early and was treated for some years by a quarterly implant under the skin before allegedly killing him – though I’m far from convinced that that was the cause of his death.
All this is irrelevant pending diagnosis, but nonetheless a worthwhile thought process if it prevents you panicking and developing a thought process to handle every eventuality. That way you are never surprised.
24 Feb 2014
So then, had the blood tests. Won’t know the PSA test results for a day or two, but much as expected I have type 2 diabetes, with a nice little extra thrown in for good measure – high cholesterol and triglycerides. Evidently I’ve enjoyed too much high living and rich food, and to prevent premature heart disease I need to change my ways.
So then, tomorrow I collect my prescription for Metaformin (which prevents the body absorbing fats by suppressing glucose production in the liver) plus statins (renowned for reducing cholesterol but are, according to some reports, damaging in their own right and not necessarily an effective cure – see here, here and here), and look forward to a diet low on carbs, fats, sugars and booze. And I must get around to more walks, ankles permitting.
My reaction on hearing the news? A bit meh, but could be worse. I celebrated by cooking home-made tandoori chicken, veg curry, home-made onion bhajis, steamed rice and naan, washed down with cold water. Tomorrow it will be pork chops and plain salad, along with other raw food. Such is life.
If you are a diabetes sufferer, recommended pages here and here.
25 Feb 2014
As a diabetic I am now an important person, so they tell me. I wasn’t important before, but now I am so I must be taken great care of. Henceforward I will be monitored with no little distinction, proactively and through appointments to see the diabetic nurse.
So then, this is the diabetes kit, pictured below. It consists of a testing kit with a book to record my blood sugar levels, an online course, two lots of meds (plus one more meds, Gliclazide, on a separate prescription) and a bewildering array of detailed instructions and advice, much of it verbal. Oh, and lots more bureaucracy to get refunds on my prescriptions too, free prescriptions being one minor benefit of being an important person.
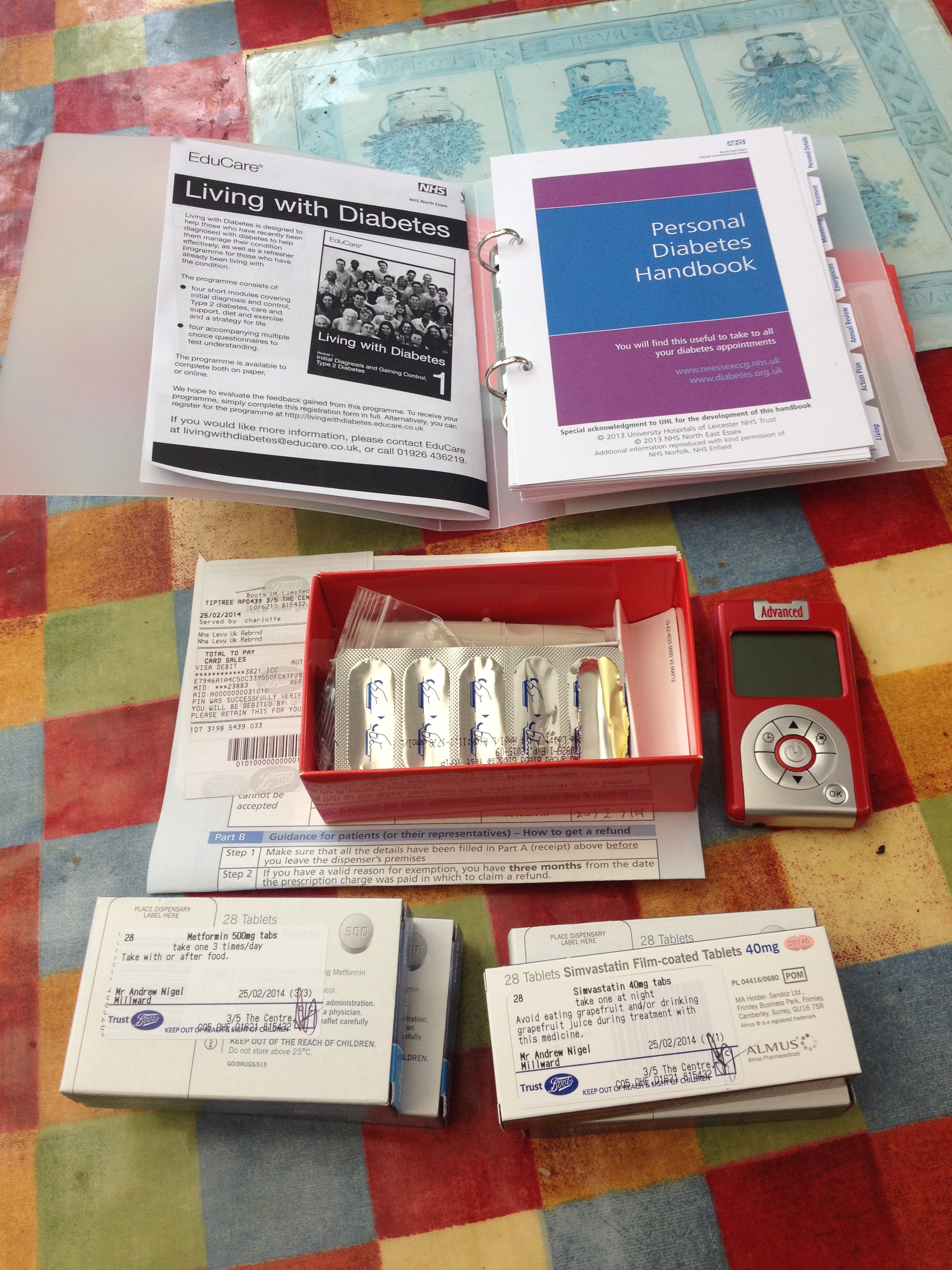 Yes, the testing kit is a pretty funky red colour and does look like an iPod, I agree! However, the meds must wait until after I give blood tomorrow.
Yes, the testing kit is a pretty funky red colour and does look like an iPod, I agree! However, the meds must wait until after I give blood tomorrow.