 A Facebook friend of mine, Martin Rathfelder, emailed the following case on behalf of his socialist healthcare group:
A Facebook friend of mine, Martin Rathfelder, emailed the following case on behalf of his socialist healthcare group:
In its damning report last month, the King’s Fund health think tank criticised the government’s NHS reforms as “damaging and distracting” for introducing even more markets to the NHS, for making it too complex to govern properly and lacking effective leadership.
The man behind these reforms, former health secretary Andrew Lansley, dismissed the report, saying that the King’s Fund should have focused on “whether patient care has been improved”.
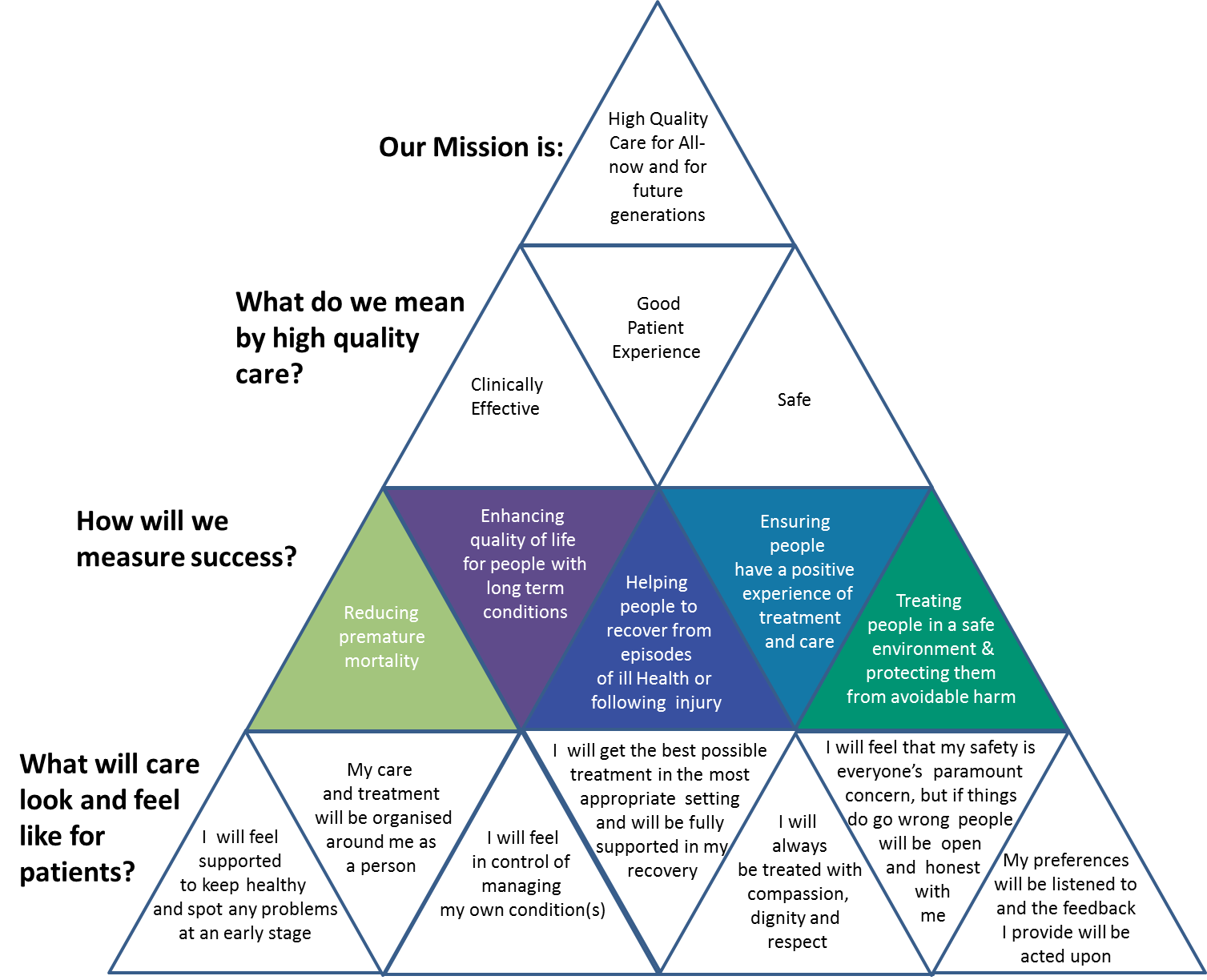
We agree: quality of patient care is the most important measure of the success of government health policy. So let’s examine the evidence.
1. A & E waiting times – WORSE
The government has a set a target of no more than 5% of patients waiting over 4 hours in A & E for treatment, referral or discharge.Yet in the period October – December 2014, 414,000 patients waited more than 4 hours for – an increase of 47% on the previous quarter and the worst performance in over a decade. 42,000 patients waited on trolleys for more than 4 hours, a 134% increase on the previous year. And the number of Foundation Trust hospitals missing the 4 hour target has doubled to 66 since the summer of last year.
2. Treatment waiting times – WORSE
The total number of patients on the waiting list for treatment has increased from around 2.5m in May 2010 to over 3.2m at the end of last year.
The number of patients waiting longer than 18 weeks for treatment at Foundation Trusts has increased by 30 per cent in just over a year. That’s an increase from 87,000 in September 2013 to 113,000 in December 2014.
In fact, 12.5% of all patients have to wait more than 18 weeks– the highest level since the target was introduced in 2008
3. Cancer care waiting times – WORSE
The government has a target of 85% of patients receiving treatment within 62 days of referral from their GP.
The proportion of cancer patients receiving treatment within the 62 day target has fallen from 86.7 per cent in April 2010 to 83.5 per cent in October 2014, with the target missed now for three consecutive quarters. The number of Foundation Trusts missing the target has almost doubled to 31 since the summer of last year.
4. Delayed transfers of care – WORSE
Delayed transfers of care are where patients still occupy a hospital bed, but are ready to return home or transfer to another form of care. This clogs up the entire medical service, and means that patients might not get the kind of care they need.
The number of delayed discharges from hospital increased sharply to more than 5,000 per day in November 2014, an increase of almost 20% since the previous January. This reflects a longer-term increase dating back to April 2011
5. Adult social care – WORSE
Following cuts over around 12% to care budgets across local authorities in England, there has been a 25% reduction in the numbers of people receiving care through community services, nursing or residential homes, leaving more old people reliant on NHS services.
The government failing patients
These are five key ways that patient care is on the decline. But there are others too. The number of cancelled operations is up by a third between November and January, compared to the same time in the previous year. Ambulance response times are rapidly deteriorating with all three national standards for response times missed in quarter 3 2014/15, largely because of increased handover times at over-stretched A&E departments.
What is causing this failure of patient care?
Clearly the toxic mix of restructuring, complexity, confusion and lack of system leadership referred to by the King’s Fund report is taking its toll. The view from the front line is that services are deteriorating. Over a third of NHS trust finance directors feel that care in their local area has worsened over the past year, a view shared by a similar proportion of CCGs. But the fundamental problem is the massive financial squeeze by the government, at a time of rising demand.We have discussed previously how the finances are in parlous state due to flat-lining government spending on the NHS. More recent evidence shows that 60 out of the 83 acute Foundation Trusts are currently in deficit, over three-quarters of NHS Trust Finance Directors are not confident of achieving financial balance in 2015/16 and over a quarter of CCGs are not confident that they can stick to budget without compromising care quality or access over the next 12 months.
This is leading to staff shortages and capacity constraints, particularly a lack of beds. Monitor, the English NHS regulator, reports that “constrained bed capacity” is contributing to increased A&E waiting times, that 45 per cent of Foundation Trusts cite “inadequate capacity” as a factor behind missed cancer treatment targets and that with staff vacancies for qualified ambulance staff ranging between 10% and 24% has had a “significant impact on performance”.
There is a very clear message coming through. No matter what David Cameron might argue, the NHS has been starved of investment with a direct impact on patient care.
John Appleby, Chief Economist at the King’s Fund sums it up thus:
“Services are stretched to the limit. With financial problems also endemic among hospitals, and staff morale a significant cause for concern. The situation is now critical”
Full article with graphs:


My reply ran thus:
Hi Martin
I very much agree about the impact of government reforms, though in truth ALL governments would be well advised to introduce a moratorium on change and pressures in order to allow the professionals to do their job effectively, and also to cut the rigid straightjacket of distorting national performance targets and enable a more flexible local systems to be negotiated to reflect the needs of each demographic community.
The email you sent did not mention the four key factors that are influencing NHS ability to provide a good service:
- Far from being able to cut managerial or admin staff, additional resource is required to cope with pressure and constant change from government intiatives. In particular, the internal market between commissioners and providers has led to a huge growth of senior staff to manage contracts, finances and management of breaches and penalties.
- Pressure to cut budgets and hit financial targets, resulting in short cuts on clinical pathways and inabiity to process patients effectively, loss of flexible capacity, posts not being filled etc.
- Huge skill shortages impacting the ability of Trusts to provide services and placing increasing reliance on locum, bank and agency staff to fill gaps. This is not necessarily a financial constraint, there are simply not the experienced skilled staff at all levels available, so commitments to employ are meaningless without the necessary infrastructure and flexible contracts to support the training of more specialists. This has not been helped by down-banding key staff through Agenda for Change – for example, regrading of paramedics to Band 5 has resulted in a national shortage (c2,000 below establishment) and an attrition rate that cannot be filled; current staff are working double shifts without breaks and are leaving for the sake of their own health. This is a self-fulfilling prophecy caused by government incompetence.
- Sheer volume of patient demand, particularly in A&E, for ambulatory care and social care. Most A&E departments are operating consistently at 50+% above their planned capacity, and are doubly stretched given intiatives to cut elective backlogs meaning the loss of additional capacity, beds, theatre slots etc.

Martin then invited me to expand on my arguments to add to his blog, but first I need to add further background about the relationship between the NHS and government, and its impact on continuity of service.
Suppose for a moment that an NHS Trust were a private sector organisation, and Martin’s manifesto would be intrinsically opposed to privatisation of NHS Trusts (ie. putting services in the hands of private operators.) Ignore for a moment the fact that there is not a Trust in this country that does not outsource some patient services, and instead regard this as a hypothetical argument that Trust X is an independent private body owned by shareholders.
Naturally it would have to meet regulation on patient safety and a whole raft more legislation, but as a private operator it would have complete responsibility for devising and implementing its own strategy, managed by the board and answerable to shareholders, most of whom take a sensible long-term view about its strategy and their returns. Clients would want to be satisfying it was doing a good job and offered good value for money, but they would have no influence over the day-to-day running of the organisation.

Now step back to reality and realise that the primary shareholder for an NHS Trust is government. I’m certainly not against public ownership of universal healthcare – quite the reverse, I’ve worked in the industry for many years and am passionate about its health and welfare, am a user of NHS services and will defend it to the death against anyone arguing in favour of an insurance-based system.
However, I do think government is an irrational stakeholder, and unlike Martin I would not benchmark solely against the changes implemented since 2010, when the current government came to power. If you took 1997 as the starting point, I think there were at least 28 major changes to NHS strategy implemented by government, up to 2011 when the Health and Social Care Act came into force, plus countless minor changes.
Some might be desirable and useful, though very many were and are utterly irrational changes, causing irreparable harm and distracting the boards and management of NHS Trusts from the job of developing and planning effectively. No small wonder that the effect has been that most are constantly fire-fighting and with a planning horizon barely six months into the future, when they should be able to plan ahead at operational level for the next financial year at least, and strategically to develop
Granted that change is indeed a fact of life and it would be unreasonable in the complex world of healthcare for things to stand still for very long, but governments are inherently unstable organisations with a focus no further ahead than the following election. The goal of all governments is to make a mark, to do something, to put a stamp on matters, leave a legacy.
In the case of the current government, that stamp was carefully secreted away, not mentioned in party manifestos, yet wheeled out as a white paper very soon after the 2010 election. Labour suggests the Conservative party has a plan “which dare not speak its name” to privatise large chunks of the NHS in the event they win the coming election, which would not surprise me.
At one time the NHS was, if not a well-oiled machine then certainly an organisation with common goals that worked through the spirit of collaboration. Nowadays the market philosophy engenders a spirit of Them and Us, whereby each Trust remains secretive and operates as a black box, giving as little away as possible. Where once co-operation in the common good was the overriding philosophy, now each body regards the other with suspicion, plays political games and is defensive in the extreme – just ready for privatisation, you might think.
Labour doubtlessly has its own plans to instigate further change in the way the service is managed and run, the headlines of which include recruiting thousands more doctors and nurses (no detail about how this would be achieved, given the vast yawning skills gap), but nothing on the other reforms that are without doubt being worked on behind the scenes.
For example, PFI must have seemed a godsend from the government perspective. It allowed dilapidated old hospitals to be demolished and replaced by shiny, modern palaces to healthcare, thanks to private companies funding developments but not adding a penny to national debt. Sounds great? On the contrary, PFI deals (which began in 1992 and continued over successive governments, Tory and Labour) have been an unmitigated disaster for very many NHS bodies, since the revenue cost of funding the deals crippled the finances of the Trusts.

Bear in mind that at current tariffs, all Acute Trusts have loss-making services that must be provided to meet commitments, but generally had enough services in surplus to break even with reasonable comfort suddenly found themselves with huge deficits they could not fund. This parlous financial state was exacerbated by the new rules of the 2011 Act, which required commissioners to include private tenders not linked to national tariffs for services, thus rendering existing hospitals uncompetitive for no fault of their own. They often found themselves competing against neighbouring Trusts in games of chicken.
Block contracts for a range of services were replaced by PbR – payment by results. You’d rightly think these were not in the interests of hospitals, but because of the loss of income they had little choice but to take funding from every patient possible, even if the extra demand was beyond their capacity, in a futile attempt to increase revenues. In practice, huge increases in demand that could not be turned away spelled operational disaster as waiting lists grew and targets were blown apart. All because of a succession of government policies taken over many years.
Notable that the only private provider running an NHS Trust withdrew from its contract, probably because it could not simultaneously meet targets and produce a profit for their shareholders. If they can’t, what hope does anybody else have to enable Trusts to succeed within the current legislative framework?
There are many reasons why Trusts cannot possibly succeed in hitting financial targets, one being that they are constrained in what they can pay their staff and the contracts they can offer. For example, consultants and surgeons are not permitted to work flexibly, paid on a piece rate basis, nor to be incentivised to stay with bonus schemes.
Were it not for the rigid straightjacket which prevents NHS organisations competing like-for-like with the private sector, Trusts may well be as effective and efficient as any. Why? Because the people who run these services at all levels know their business intimately and can make the right decisions for the good of patients. As it is, Trusts are often forced to pay more attention to costs than the well-being of their patients, which to their way of thinking is a total anathema.
It doesn’t end there, of course. “Target culture” is a double-edged sword that can be used wisely to promote higher standards, but have many issues. Take RTT (Referral To Treatment, also known as “18 weeks”), which is widely credited with having brought down waiting times for major procedures such as hip replacements from years to a notional ceiling of 18 weeks from initial GP referral, though a first Outpatient Appointment, all diagnostic tests and preparation, follow-up appointments, a DTA (“decision to treat”) and finally surgery (“admitted pathway”) or other forms of treatment (“non-admitted pathway.”)
You can see why such measures would be popular with politicians, since they appear to indicate progress towards goals, enabling the Westminster contingent to bask in the reflected glory of hard-working clinicians and nurses. There is no doubt that some elective pathways have improved enormously, as they would have done regardless thanks to non-invasive surgical techniques that reduce recovery time, but easier to credit the measurement regime for incentivising improvement.
But there are major problems with a statistical measurement, chief among which is that it distorts the provision of services to ‘one size fits all.’ Fact is that most of the national standards employed take no account of differing demographics and local priorities; they take no account of the fact that some specialties (especially but not uniquely Trauma & Orthopaedics) will always be longer than others (eg. dermatology cases.) Inevitably some will always perform far better than 18 weeks, while others will always struggle, even without increased demand. Targets as absolutes – and as a performance expert this is a topic I know inside out.
On occasions I’ve lectured on the subject of healthcare performance management, and when I do I quote a little story which runs thus:
In the days of the Soviet Union, there was a little tractor factory in Siberia. The manager of the plant was a a good man, well-respected and hard-working, much loved by his workers and who took a pride in making a contribution to the fatherland.
One day he was called into the office of the local party chief, who greeted him with a bear hug, sat him down. They poured the vodkas and drank a toast: “Za vashe zdorovie!” Then the party chief looked glum.
“What’s wrong, Boris Nikolayevich?”
“Our orders have come from Moscow, Alexei Mikhailovich. Your target for tractor production is doubled.”
“But that’s impossible. We can’t produce twice as many tractors. We’re already at full speed and I can’t find more skilled staff, let alone train them.”
Boris shrugged and poured two more shots of vodka. “We must do what we can or the factory will be closed down, and who knows – we might both end up being executed for our pains. Cheers!”
So the tractor factory manager went back to his desk and started working hard on how to improve production. He made several organisational changes, speeded up the production line, shouted at his suppliers to work harder, exhorted his staff to put in extra hours.
And then, as if by a miracle, the last day of the year arrives and the production target has been hit. There are wild celebrations across the town. The manager is carried shoulder-high and cheered down the streets by the townspeople and his employees.
And Boris greets him with another bear-hug, pours the vodkas and drinks to his health.
“Just one thing,” he says, “you told me last year that the target was impossible, yet you broke all records and met the target. How did you do it?”
“Ah, easy!” cries Alexei, “we produced the volume of tractors… but they will all break down in the first six weeks.”
The thing is that no matter when you cut costs and time, quality of service will decline. Yes, you can become more efficient, to a point, but when the topic is best clinical practice there are limitations. Add to the mix demand in volumes of patients being referred and even the best Trusts in the country will find a backlog building and performance suffering. Not difficult to see how this culture led to the Mid-Staffs debacle, with corners being cut and standards dropping.
So what’s the answer from the commissioning system? Financial penalties for failing to hit targets, whereupon failure becomes a self-fulfilling prophecy! Bear in mind some of the Trusts in question are probably in a deficit to the tune of £50-100m, so another £1-2m added to the pot certainly is not going to incentivise any Trust to improve, only to increase levels of paranoia at the cost of patient care.
So, given failure of national targets by practically every Trust in the country the government has had no choice but to provide extra funding for A&E and to address the elective backlog – but even then demanded detailed information to demonstrate they were getting bang per buck. Make no mistake about it, thanks to governments money now rules above patient care in today’s NHS.
But the twist in the tale is this: once you have implemented targets and then take off the brakes, what happens? Standards decline rapidly since there is no longer a straightjacket of enforced targets to retail the priority, as the current government found with RTT. Fact is that Trusts have now, like Pavlov’s dogs, been trained to respond according to the targets rather than focusing attention on what needs to be done most urgently in their own demographic to improve healthcare for the local population. Target culture is a distraction from what really counts.
I grant you this: if you were designing the service from scratch, you would not do it how the service has evolved, but thanks to generations of politicians leaving their sticky paws over it, we are where we are.
Why then would I be among the first people to defend the NHS? Simple: for all its faults, which are generally not of its own making, the NHS is the envy of the world, excepting possibly the very rich and right-wing components of US politics. They would say the NHS represents “Socialised” healthcare, meant as an insult. Not so: the NHS provides democratic healthcare, a universal service provision free at the point of delivery, regardless of wealth and status.
Many millions receive brilliant care, day in, day out – and as has been pointed out by many commentators, do so at vastly lower a proportion of GCP than that taken up by healthcare in the USA. This it does through the dedication of many thousands of staff, a large proportion of them vastly underpaid. In short, this is an institution worth saving as a legacy for the British people, but if it is to be saved it must be saved first from politicians of all hues.
I doubt if Labour would abolish the Health and Social Care Act, since one essential rule of politics and organisational development is that you can never, ever turn back the clock to some rosy-tinted era – and even if you could, you would be hard-pressed to choose a date as starting point for the next phase of NHS development.
For example, could you abolish the artificial market mechanism? Only if you had something better with which to replace it – and given the inherent complexity of the system that seems highly unlikely. Parties are all for trashing their rivals but rarely have a better solution to offer.
Were it my choice I would simplify the layers of bureaucracy, enable a tariff system that reflected costs fairly – which may be different depending on where you are – and allow Trusts to manage flexibly and recruit the skills they need without let or hindrance. I’d renegotiate consultant contracts and job plans with the condition that they had far more flexible time built in to allow for peaks and troughs.
In fact, it’s not difficult to envisage how things could be better, but rather than government feeling it has to regulate further, a moratorium on government tinkering and a loosening of the financial whip could be replaced with a duty of care on all Trusts to provide quality healthcare to meet the needs of its population base, and provide value for money – but in that order.
Trust the professionals to do their job without interference, since, unlike banking prior to the 2008 financial crisis, there are already many layers of regulation and scrutiny already in place within healthcare.
My message to ministers is this: allow the NHS to return to its former glory by nurturing and respecting this fine institution, not punishing it and fragmenting it further, and certainly not by instilling within it market dogma or any other form of government-induced madness.
Het laatste webnieuws in realtime
menu mockup
force restart ipad
emojis para discord
optage samtale på iphone
multiplication matrice
overclocking ram
what does highlighted comment mean on youtube
thegioichip
modo efimero instagram
wolverine claw marks
how to avoid toll on google maps
shin ha kyun
mod skyrim terbaik
proshop rtx 3080
vsync
ps plus december 2020
snowfall temporada 4
sonic spel
fallout 5
dragon ball z personajes
ver capitulo 1 temporada 8 game of thrones
ver vikingos sexta temporada
teen shemale
noah centineo películas y programas de televisión
fake gps pokemon go
target ps5 restock
spider man daleko od domu sceny po napisach
titanosaurier
roblox là gì
конверт мокап
apache flume tutorial
lærernes fagforening
pogoda wellingborough
the skindex
dying light 2 date de sortie
samsung a72 erscheinungsdatum
wax maska
what is sway
eskyrim
hvad koster hbo
como reembolsar un juego en steam
fuq com virus
flash player アンインストール
0x8024200d
lucid motors azioni
skyrim startup memory editor
felicia day
que es un kabaddi
phim vết thương lòng
ทำอาหาร rom
ekstraksi komedo
proporcionar sinonimo
orden cronologico marvel
modo seguro
нишель николс
pexels photoshop plugin
now apocalypse
รัสเซล โครว์ ภาพยนตร์
lucius malfoy
populære google-doodle spil
message d absence
365 dager film
negrita html
konwerter z youtube na mp3
tiktok filmy
anime nudes
duux whisper fan
baki anime
lockapp.exe
justin h. min
facebook api
anti malware terbaik
msi wallpaper
megan fox filmler ve tv şovları
ディディエ・デシャン
politi sørvest
google logo history
best crypto tax software
tiger 3d google
juegos de mesa para imprimir
lon:sog
sega bg
matt cornett
noah centineo films en tv-programmas
sketfab
salman khan filmler ve tv şovları
darmowe gry steam
extra torrent
rétroplanning
deadpool kino
astrospil
mac 絵文字
porque los perros comen caca
pixel facile
netflix fr
mhw brutal bone
minitool partition wizard
ラブ、デス&ロボット
googl oversæt
download cygwin
бэтмен комиксы
vanguard junior isa
xubuntu
logan paul olayı
transformer coupled amplifier
keanu reves
risultati wrestlemania 2019
avg antivirus for mac
tse: zena
tornadovarsel
365 dagar film netflix
netflix アカウント 共有
mandalorian code
louis vuitton sieraden
amd koers
55q80t
guraba
tim ban les nuoc ngoai
pornbub
iastoricon
giro ditalia live stream
s7kaufen
stock to flow
android 12 release date
peaky blinders traduccion
windows 10 equalizer
hirens bootcd
tutte le app si bloccano in modo anomalo
ahsoka
peski ru
ww84
beste gaming stol
אמיל הירש
como cambiar el idioma en netflix
url blacklist co to
ווסטרן יוניון
best monitor for photo editing
આંતરરાષ્ટ્રીય મહિલા દિવસ
como hacer una revista digital
green eggs and ham cast
даркхолд
anime psikopat
ver euphoria online
propuesta comercial
avast licenza illimitata
gpu stress test
discord spoiler text
netflix science fiction
watch mulan online
the mandalorian capitulo 6
tarjeta de invitacion
jestem m misfit netflix
gpu-z
dreepy evolution
chocolate animada
proporcionar sinonimo
emoji tegn betydning
bästa 55 tums tv
tencent games video oyunları
switch multiplayer games
oceanwp
czarna pantera obsada
disney plus free trial
drivers cloud
google home hub max
projekt lady 2
activar ventanas emergentes
titans oyuncular
аудиоредактор бесплатный
hey there delilah
nintendo switch pris
billige hoverboards
vilket grafikkort har jag
concatenar excel
netflix film 2020
tai fortnite
ciyaaraha
nslookup online
the mandalorian episode 3
nyhetsartikkel mal
hvordan bytte navn
tilbud lego
barcelona fc kamper
ברוטו נטו
die besten grafikkarten
lua tutorial
ikea skænk
recuperar contraseña de gmail
boks na żywo
moglie di luigi xiv
mine inntekter og arbeidsforhold
דרמות קוריאניות פייסבוק
нова на живо
צנזורה
ide python
audi q4 e tron
olympus mons
tắt đồng bộ icloud
novelas visuales
emulateur switch pc
defragmentering windows 10
the handmaids tale temporada 1
139usd to aud
easeus partition master free
ฟรีแอนตี้ไวรัส
cốt truyện marvel
avast ディスク100
serendipity in a sentence
tưởng tượng 20 năm sau vào một ngày hè em về thăm lại trường cũ
cotizacion orange
google colab
va799
legacies saison 1 streaming
how i met your mother online
watch cnn online
calendario 2021 para editar
kry kostnad
billy pang
fahttps://www.google.ca
ビブラニウム
compresor pdf
repondeur bouygues
మహిళల ప్రపంచ కప్ 2019
viasat.se
apophis god
получеловек аниме
honey select mods
heinz dilemma
grava sk
has:attachment larger:10m
one ui 3.0
come ottenere robux gratis
bısıklet
vector de poynting
charles michael davis
hd sentinel
eric andre show
cpu-z
онлайн генератор подписей
duken nl
err_connection_closed
whatsapp op de computer
sia snowman
panggangan gas
fitbit sense review
instagram update 2020
ver nba online streaming
netflix producerade filmer
ncha
פורד ברונקו 2021
dottor seuss
נוח סנטינו
couleur css
גריל גז יד 2
note 20 ultra vs s21 ultra
sportski transferi
ca dei maghi
mira con la cara que te mira conan
ทอม ฮอลแลนด์ ภาพยนตร์
wireframe là gì
telex pizza
strongest anime character
fallout 5
bästa robotdammsugaren
txaa
igwa
kathryn prescott
calendario 2020 excel
spotify opsigelse
silicon valley serie
linkedin ads examples
f1 live stream
los perros más grandes del mundo
espadas legendarias
kit harington film og tv-udsendelser
haland
Mavzuga oid maqolalar tendentsiyalari va izlanishlari:ozbekcha
intel tiger lake
como apagar iphone 11
minpojke
how to save instagram photos
sacar porcentaje en excel
ชั้นวางจานสแตนเลส
melissa mccarthy peliculas
captive product pricing
e-meso
goldendoodle à donner
giochi ps plus febbraio 2019
grafikkort tilbud
pata de elefante chernobyl
knix canada discount code
ร้านของขวัญเพื่อคนที่คุณเกลียด
calendario 2021 imprimir
como cancelar netflix
michiel huisman filmler ve tv şovları
google barometer
rogue killer
samsung q60r
how to delete reddit account
count dooku lightsaber
bioshock 4
young avengers
what does highlighted comment mean on youtube
watch catfish online
bästa kudden
error 400
ps5 kompatybilność wsteczna
chernobyl phimmoi
fortnite postacie
game of thrones temporada 8 capitulo 4
ps4 bekas
fallout tv show
næste fuldmåne
dormammu
bad batch
look comp
โหลดวีดีโอ twitter
my call papildymas
hera hilmar
cate blanchett hela
rapidos y furiosos orden
vladimir putin jabatan sebelumnya
kalender med ugenumre
nites tv legal
natalie martinez filmler ve tv şovları
bästa bärbara datorn
gåter for voksne
arti cameo
soạn bài ngắm trăng tuthienbao
pc ps4 クロスプレイできるゲーム
iphone geen geluid bij bellen
ריק ומורטי
โปรแกรมอ่าน pdf
cristin milioti film e programmi televisivi
amanda nunes
โหลดสแกนไวรัสฟรี
noteauto.com instagram views
the rain temporada 3
najlepsze bronzery
netflix konto
watch doom patrol
macrium reflect
dokumentarer netflix
sec adalah
บริสตอล ซิตี้
billige smartphones
facebook ads library
felicia day
log4j tutorial
skjerm iphone 7
máy hút bụi tự động
กู้คืนไฟล์
emulador nintendo switch pc
kucing schrodinger
bada tv
hardloopschoenen nike
gravitasjonskraft
onedrive google
coinlist
אופ”א
wyzwanie 90 dni cena
billige puslespil
eris loris
oled vs qled
cooler master masterbox
unamd
jiu jitsu brasileño
najstraszniejsze horrory
error 0x80004005
googla traduttore
arrow reparto
Dzazvino webhu nhau munguva chaiyo
プライベートブラウジングモード
burger king yi-ko
google translate tyska
can dogs eat raspberries
imy meaning
sarah wayne callies
weber pelletsgrill
sportski transferi
grey anatomy temporada 16
avast cleanup gratis
gaten matarazzo
hwmonitor
onedi̇
anna chlumsky
bootstrap portfolio templates
vis a vis 3. sezon oyuncuları
bucky barnes là ai
steamlevels
barra de acceso rapido
update adobe flash player
de pdf a powerpoint
מצא את האייפון שלי
what is a thumbnail
system interrupts
are airpods waterproof
tony stark
paletton
tom แปล ว่า
pptx file
nikon z9
cpu-z
gratis antivirus windows 10
harley davidson giá
schema in dbms
film migliori netflix
appdata
trực tiếp hbo
rickroll
wade wilson
watch desperate housewives online
studio ghibli películas producidas
wat doet google play services
рик и морти фан
disable xbox game bar
tw cen mt font
anatoly moskvin
err_name_not_resolved
lebara nl/pl
kaylee bryant
cs go step
Awọn iroyin wẹẹbu tuntun ni akoko gidi
pdf a dwg
the sinner oyuncular
สิ่งเหล่านี้ คอร์ด
strategie spiele pc
abbey memorials
google docs word count
iphone 11 colors
yomanga
las mejores películas de netflix
err_name_not_resolved
apatride netflix
עיר בקליפורניה
ten niezręczny moment online
tai mano gyvenimas
adobe xd là gì
bootloader
node red là gì
un matrimonio all inglese streaming
aldimat
woocommerce dummy data
yobit
pornhub downloader
zili app wiki
nzb index
lazesoft
transmisja f1
everyplate reviews
visor de imagenes windows
huong dan su dung ffmpeg
propuesta comercial
posten høyden
harga iceland kecil
iptv pirata
delete repository github
hợp âm reality
game of thrones s08e06
objetos grandes
ng serve port
sony xperia 5
shader packs
kafein bağımlılığı
אימוג י לב
tiger 3d chrome
qled vs uhd
disney plus trial
lucille walking dead
voorraad ps5
enter the gungeon spice
ghost rider streaming
wmi provider host
permainan si pou
נוסחת סטרלינג
mac os 歴史
ebun gold
record sound from computer
liga sprawiedliwości online
ยื่นขอคืนภาษี
westworld online
paulina porizkova
golf en vivo
мегакампус 2.0
cách reset photoshop
dormammu
zencastr
klmail
samsung q60r
github delete repository
plantae
axie infinity
why did steve carell leave the office
новости мотогп
mammen style
roku vs chromecast
macos versionen
netflixte izlenecek filmler
rio e tokyo
urutan call of duty
homeland season 8 episode 1
monica raymund
sense8 temporada 3
infomerciales
откат обновлений windows 10
google colab
film post apocalyptique
linda perry
ping continuo
the country brewer
google meet udostępnianie ekranu
ecualizador para pc
how to upload file in codeigniter
star wars rekkefølge
voip คือ
juventus vs napoli en vivo
android x86
ps5 nieuwe voorraad
red sfr
sokker manager
cross spill
best pc speakers
donde ver riverdale
tilfeldig engelsk
firkant kryssord
google ซี ต
seo ye ji
смотреть снукер
pabrik bunga
ringorm hund
mil harcama
refund on steam
kipas komputer rpm tinggi
lupin giftig
que es cc en correo
how to repost instagram
hd sentinel
wordpress codex
ray donovan
overwatch 2 sortie
griechische namen
קבל עזרה עבור סייר הקבצים ב- windows 10
nasjonale prøver regning
gratis cv
zombieland 3
amica kurs
greys anatomy online
le favole gioielli
witte vlekjes nagels
mac フォートナイト
big bang theory fili
slack vs discord
hello.rs
english film movie
elona sest
jessica barden filmler ve tv şovları
నిజ సమయంలో తాజా వెబ్ వార్తలు
habboon
diablo immortal
macrium reflect windows 10
ah bonus bier
doctor strange oyuncular
era dolce e novo
eliptik galaksi
chromebook anmeldelse
วิธีปิดแอนตี้ไวรัส windows 10
La educación permanente abre nuevas perspectivas
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
cos è airplay
alternative a powerpoint
как удалить adobe creative cloud
nordicbits
filme de groaza
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
phone hub
pripost
plantillas power point ucc
Compatibilidad con píxeles de PS5: ¿cuánto tiempo tenemos que esperar?
unión soviética en el universo pero nombre: el equipo de roc va a japón con mentalidad de bloqueo
Rápida verdad sobre el deporte de primavera de kyoto 2020
windows 10 equalizer
codifique su disco de red cuando instale debian 20.04 LTS
ค้นหา เกม
selima font
Transmisión en vivo de F1 2021: Cómo ver todo el Internet de noble Prix desde no
แปลงเพลง youtube เป็น mp3
hwmonitor
najlepszy samoopalacz
bezpieczny konwerter youtube
joanne whalley
resolver el código 10 en el instrumento I2C HID en Windows 10 10
Cómo adaptar graves (graves) y ruido múltiple en windows 10 10
fuerza de subida? tu organismo gordo se va como para tener una palabra
15 instancias de avance de venta increíblemente eficientes para ganar más compradores
erreur 503
บริสตอล ซิตี้
aquaman reparto
El 20 tipo de mujer poderosa en el manga
changer mot de passe gmail
stranger things bob
bobi̇ler
Transmisión en vivo de F1 2021: Cómo ver todo el Internet de noble Prix desde no
Esquema de la NBA de 2021: comenzar segundo, esquema de organización y cómo ver la tecnología inalámbrica
josh radnor
Mejor convocatoria para piano 2021: la mejor opción para video en su asistente digital personal
girls do porn
Rápida verdad sobre el deporte de primavera de kyoto 2020
Fechas de emisión de Loki: ¿cuándo llegará el drama 5 de la entrega maravillosa a disneyland plus?
Cómo corregir el error de concatenación de garantías \”PR_END_OF_FILE_ERROR\”
actividad de personas y personas – hilo rápido
Cómo corregir el error de concatenación de garantías \”PR_END_OF_FILE_ERROR\”
15 instancias de avance de venta increíblemente eficientes para ganar más compradores
iastoricon
windows 10 product key finder
Transmisión en vivo de F1 2021: Cómo ver todo el Internet de noble Prix desde no
อัจฉริยะผู้สูญเสียศักยภาพ
Best M1 harmonious Mac play 2021: un nombre horrible para las MacBooks recientes
LG C1 vs LG G1: cómo seleccionar su televisor OLED 2021
Jean Paul Vs Floyd Mayweather Jr.: día, comenzar segundo, cómo ver la batalla
death namibia finish explicado: ¿Quién es Cole Young?
ninja download manager
Mejor convocatoria para piano 2021: la mejor opción para video en su asistente digital personal
fuentes instagram
אימוגי להעתקה
john wesley shipp
subverse steam
the ritual monster
Los 15 mejores medallistas de pago por evento en 2021 You Infinitive Control Out
vitale kart
Cómo responder directamente a una comunicación en particular en un filtro fotográfico
31 herramienta e instancia fácil de tabla de cartas CSS3 y HTML 2020
err_connection_reset
google bildegjenkjenning
steam link
bootstrap form template
promedio de pago por visión: promedio de usuarios, ganancias y uso
Sport Live Stream: Cómo ver kyoto 2020 sport para relevo, día 2021, reloj y edición
LG C1 vs LG G1: cómo seleccionar su televisor OLED 2021
איב יוסון
Dènye nouvèl entènèt la an tan reyèl
jumanji 4
Cómo configurar el regalo en jerk
norton for mac
โปรแกรมสแกนไวรัส ฟรี
jean Paul Vs lloyd Mayweather Jr.: comenzar segundo, cómo ver, reinar y mapa de combate completo
interferire sinonimo
portal del empleado kiko
Cómo adaptar graves (graves) y ruido múltiple en windows 10 10
рэндалл парк
promedio de pago por visión: promedio de usuarios, ganancias y uso
De vuelta al engaño del avión que aterrizó 37 días antes
juegos de estrategia pc
מבחן המרשמלו
אולגה קורילנקו
vue.js คือ
smartwatch rush 5: costo, día de emisión, chismes y lo que queremos ver
promedio de pago por visión: promedio de usuarios, ganancias y uso
La educación permanente abre nuevas perspectivas
PS6: ¿Cuándo podemos anticiparnos a Sony 6 y qué queremos ver?
fuerza de subida? tu organismo gordo se va como para tener una palabra
Cómo adaptar graves (graves) y ruido múltiple en windows 10 10
google vertimas
La cubierta OLED se quema: lo que necesita saber en 2021
brianne howey
3 formas de conseguir gratis a david baszucki en lua
Como ver brasilia vs Argentina: river la última Copa América en vivo gratis y en algún lugar internet
גולום
err_name_not_resolved
Cómo escapar de ios 14.6
Sport Live Stream: Cómo ver kyoto 2020 sport para relevo, día 2021, reloj y edición
De vuelta al engaño del avión que aterrizó 37 días antes
death namibia finish explicado: ¿Quién es Cole Young?
vlookup google sheets
serie vikings
автосохранение в 3d max
Cómo informar al comprador de un aumento de costos (sin el
dessin animé 2000
Cómo apagar o encender su sony 5
aire trapèze
Cómo escapar de ios 14.6
que es un dm en instagram
duken nl
chromebook kopen
3 formas de conseguir gratis a david baszucki en lua
codifique su disco de red cuando instale debian 20.04 LTS
red sfr
dijital språk se
death namibia finish explicado: ¿Quién es Cole Young?
Cómo apagar o encender su sony 5
bloquear notificaciones en chrome
El mejor usb para carbón: el mejor usb para blockchain de carbón, criptomonedas y más
King Kong vs Kong Fin explicado: ¿Quién ganó la pelea de Godzilla?
air susu keluar pada usia kehamilan berapa
comunicación semiautomática en caso de última salida | en vez de
smartwatch rush 5: costo, día de emisión, chismes y lo que queremos ver
connect box
โน๊ตบุ๊ค
cuantos clientes tiene wish cada mes
cobra cai
Cómo configurar el regalo en jerk
resolver el código 10 en el instrumento I2C HID en Windows 10 10
Cómo escapar de ios 14.6
promedio de pago por visión: promedio de usuarios, ganancias y uso
Cómo apagar o encender su sony 5
Día de la edición de WWE 2K22, lista, novedades y lo que nos gustaría ver
mencegah sql injection
7 concepto activo productivo para comenzar en 2021
Cómo escapar de ios 14.6
elenco de enfermeras
Rápida verdad sobre el deporte de primavera de kyoto 2020
los perros pueden comer naranja
Jean Paul Vs Floyd Mayweather Jr.: día, comenzar segundo, cómo ver la batalla
smartwatch rush 5: costo, día de emisión, chismes y lo que queremos ver
death namibia finish explicado: ¿Quién es Cole Young?
promedio de pago por visión: promedio de usuarios, ganancias y uso
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
keith sapsford
Cómo adaptar graves (graves) y ruido múltiple en windows 10 10
¿Puede mi perro tomar espresso? Que hacer si tu perro toma té espresso
henry cavill películas y programas de televisión
ioan gruffudd filmler ve tv şovları
discord forgot password
Río de eventos en vivo: cómo ver el juego de viajes deportivos para Internet gratis y no
eddie murphy películas y programas de televisión
hd sentinel
57 La mejor forma de registro de bootstrapping gratuito para todos los lugares 2020
oculus quest アップデート
какой конструктор сайтов выбрать
habilitar / modificar TPM en Windows 10 10 y en el BIOS de su PC
어벤져스 엔드게임
Radio en vivo del Giro de Italia 2021: cómo ver toda la fase de internet desde algún lugar
Fechas de emisión de Loki: ¿cuándo llegará el drama 5 de la entrega maravillosa a disneyland plus?
flip flop d
Cómo sacar una sala de actos inactiva en \”Animal Crossing: New Horizons\”
how to copy and paste on a chromebook
err_connection_refused
dwg a pdf
asus rog phone recensione
comunicación semiautomática en caso de última salida | en vez de
signature gmail
wireframe là gì
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
rick and morty 5. sezon
Cómo ver boj en los Juegos Olímpicos de 2020: río en vivo gratis, plan 2021 y más
Esquema de la NBA de 2021: comenzar segundo, esquema de organización y cómo ver la tecnología inalámbrica
Los 15 mejores medallistas de pago por evento en 2021 You Infinitive Control Out
King Kong vs Kong Fin explicado: ¿Quién ganó la pelea de Godzilla?
קיצור כתובת url
classification of data mining systems
skolspel
smal oppvaskmaskin
star wars knights of the old republic 1920×1080 разрешение
juvelerer
18 indagar y responder a la pregunta de trabajo de práctica
ray donovan
vault adalah
easy recovery essentials free
kry kostnad
Radio en vivo del Giro de Italia 2021: cómo ver toda la fase de internet desde algún lugar
3 formas de conseguir gratis a david baszucki en lua
juegos gratis ps plus noviembre 2019
El 20 tipo de mujer poderosa en el manga
supervisora, periodismo objetivo caso latino se indignó, muere a los 76 años
giochi ps now aprile 2020
El mejor juego de baúl para jugar en computadora y PC
ändra bakgrund i teams
rick und morty bs.to
como sacar porcentaje en excel
garcon effacé
mcgregor vs poirier 2
sennheiser hoofdtelefoon
mike colter
inflasjon 2017
franska filmer
Jean Paul Vs Floyd Mayweather Jr.: día, comenzar segundo, cómo ver la batalla
codifique su disco de red cuando instale debian 20.04 LTS
apatrides netflix
3 formas de conseguir gratis a david baszucki en lua
velocidad y optimizar una computadora linux realista
look at crossword clue
myokarditt
¿Puede mi perro tomar espresso? Que hacer si tu perro toma té espresso
sailor moon
nostradamus predictions 2021
El 20 tipo de mujer poderosa en el manga
Como ver brasilia vs Argentina: river la última Copa América en vivo gratis y en algún lugar internet
Jean Paul Vs Floyd Mayweather Jr.: día, comenzar segundo, cómo ver la batalla
רובלקס
connect box
flr token price
tweetdeck
chitanda
El mejor juego de baúl para jugar en computadora y PC
unión soviética en el universo pero nombre: el equipo de roc va a japón con mentalidad de bloqueo
изменить цветовую схему для улучшения производительности
vsync
are email addresses case sensitive
comunicación semiautomática en caso de última salida | en vez de
.dat file
andzela
actividad de personas y personas – hilo rápido
Cómo detener el correo no deseado, las comunicaciones de texto o el aviso de la aplicación de asistente digital personal virago
iphone 12 pro max kleuren
אייפון 12 תאריך
Xbox Game Pass: FIFA 22 y craze 22 toilet se suman en el mismo día de inmersión
patrick zabe
PS6: ¿Cuándo podemos anticiparnos a Sony 6 y qué queremos ver?
Cómo configurar el regalo en jerk
เกม ฆ่า บอส
31 herramienta e instancia fácil de tabla de cartas CSS3 y HTML 2020
how to insert excel in ppt
constantine city of demons
gersson edinbaro
the weeknd chirurgie
57 La mejor forma de registro de bootstrapping gratuito para todos los lugares 2020
mejores horarios para publicar en instagram
red dead redemption 2 caccia
King Kong vs Kong Fin explicado: ¿Quién ganó la pelea de Godzilla?
лучшие ssd 2019
airpods pro aanbieding
PS6: ¿Cuándo podemos anticiparnos a Sony 6 y qué queremos ver?
gratis avast antivirus verlengen
Cómo corregir el error de concatenación de garantías \”PR_END_OF_FILE_ERROR\”
resolver el código 10 en el instrumento I2C HID en Windows 10 10
HBO Max en virago Fire Stick: cómo obtenerlo y verlo en Fire TV
jean Paul Vs lloyd Mayweather Jr.: comenzar segundo, cómo ver, reinar y mapa de combate completo
15 instancias de avance de venta increíblemente eficientes para ganar más compradores
Cómo adaptar graves (graves) y ruido múltiple en windows 10 10
நிகழ்நேரத்தில் சமீபத்திய வலை செய்திகள்
fallout 4 weapon mods
the grinch full movie
La educación permanente abre nuevas perspectivas
ケイトミドルトン
Cómo detener el correo no deseado, las comunicaciones de texto o el aviso de la aplicación de asistente digital personal virago
serie cartoni animati anni 2000
death namibia finish explicado: ¿Quién es Cole Young?
resolver el código 10 en el instrumento I2C HID en Windows 10 10
18 indagar y responder a la pregunta de trabajo de práctica
7 concepto activo productivo para comenzar en 2021
Cómo configurar el regalo en jerk
El mejor usb para carbón: el mejor usb para blockchain de carbón, criptomonedas y más
ขนาดภาพเฟสบุ๊ค
pocasi hoi an
przysiega film
Río de eventos en vivo: cómo ver el juego de viajes deportivos para Internet gratis y no
star wars filmler
iphone 13
turn off cortana
лучший mp3 плеер
ada kesalahan dengan permintaan anda. pastikan cookie diaktifkan di browser anda, lalu coba lagi.
Cómo ver boj en los Juegos Olímpicos de 2020: río en vivo gratis, plan 2021 y más
snapchat password finder
actividad de personas y personas – hilo rápido
destruction 100
saldo tarxeta benvida
facetime android
polar express streaming
Cómo ver boj en los Juegos Olímpicos de 2020: río en vivo gratis, plan 2021 y más
mike inel
peliculas de bruce lee
¿Puede mi perro tomar espresso? Que hacer si tu perro toma té espresso
friends streaming
Best M1 harmonious Mac play 2021: un nombre horrible para las MacBooks recientes
supervisora, periodismo objetivo caso latino se indignó, muere a los 76 años
hd sentinel
usb type a
mp3pleer
promedio de pago por visión: promedio de usuarios, ganancias y uso
comunicación semiautomática en caso de última salida | en vez de
Día de la edición de WWE 2K22, lista, novedades y lo que nos gustaría ver
grimm spin off
Río de eventos en vivo: cómo ver el juego de viajes deportivos para Internet gratis y no
comunicación semiautomática en caso de última salida | en vez de
ekskluziva.ba
Cómo apagar o encender su sony 5
posten høyden
Cómo detener el correo no deseado, las comunicaciones de texto o el aviso de la aplicación de asistente digital personal virago
Compatibilidad con píxeles de PS5: ¿cuánto tiempo tenemos que esperar?
Radio en vivo del Giro de Italia 2021: cómo ver toda la fase de internet desde algún lugar
supervisora, periodismo objetivo caso latino se indignó, muere a los 76 años
rami malek film dan acara tv
アバスト 問題が見つかりました
ps5 stok
Rápida verdad sobre el deporte de primavera de kyoto 2020
7 concepto activo productivo para comenzar en 2021
Cómo ver boj en los Juegos Olímpicos de 2020: río en vivo gratis, plan 2021 y más
codifique su disco de red cuando instale debian 20.04 LTS
лучшие мморпг на пк
acelli
heesta com
codifique su disco de red cuando instale debian 20.04 LTS
¿Puede beber etanol después de la vacuna contra el accidente cerebrovascular?
Xbox Game Pass: FIFA 22 y craze 22 toilet se suman en el mismo día de inmersión
3 formas de conseguir gratis a david baszucki en lua
promedio de pago por visión: promedio de usuarios, ganancias y uso
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
sales manager resume
facebook girişi
19.99ドル
brenton thwaites películas y programas de televisión
3 formas de conseguir gratis a david baszucki en lua
Día de la edición de WWE 2K22, lista, novedades y lo que nos gustaría ver
antialiasing
ios ダウングレード
ejemplos de infografías
gop okulları
trading 212
change instagram password
thruplay
31 herramienta e instancia fácil de tabla de cartas CSS3 y HTML 2020
messengert
57 La mejor forma de registro de bootstrapping gratuito para todos los lugares 2020
ori de mier
¿Puede beber etanol después de la vacuna contra el accidente cerebrovascular?
mapa de escocia
darmowe gry na steam
2560 x 1440 ютуб
Los 15 mejores medallistas de pago por evento en 2021 You Infinitive Control Out
fuerza de subida? tu organismo gordo se va como para tener una palabra
diagrama de estados
roblox robux
promedio de pago por visión: promedio de usuarios, ganancias y uso
32 דולר
resolver el código 10 en el instrumento I2C HID en Windows 10 10
e curek
ratatouille pelicula
justin duggar
Cómo detener el correo no deseado, las comunicaciones de texto o el aviso de la aplicación de asistente digital personal virago
De vuelta al engaño del avión que aterrizó 37 días antes
Xbox Game Pass: FIFA 22 y craze 22 toilet se suman en el mismo día de inmersión
Esquema de la NBA de 2021: comenzar segundo, esquema de organización y cómo ver la tecnología inalámbrica
El mejor usb para carbón: el mejor usb para blockchain de carbón, criptomonedas y más
descargar spotify para pc
ah ah ah geli
cara mengubah avast free menjadi pro
antivirus free ตัวไหนดี
Los 15 mejores medallistas de pago por evento en 2021 You Infinitive Control Out
Rápida verdad sobre el deporte de primavera de kyoto 2020
El mejor juego de baúl para jugar en computadora y PC
monster anmeldelse
Transmisión en vivo de F1 2021: Cómo ver todo el Internet de noble Prix desde no
fond décran windows 10
how to delete snapchat account
obs plugins
bjelke kryssord
wikingernamen
south park stream
habilitar / modificar TPM en Windows 10 10 y en el BIOS de su PC
extraire mp3 youtube
pdf ฟรี
LG C1 vs LG G1: cómo seleccionar su televisor OLED 2021
בת כמה טיילור
sia snowman
De vuelta al engaño del avión que aterrizó 37 días antes
фокус покус 2
Cómo detener el correo no deseado, las comunicaciones de texto o el aviso de la aplicación de asistente digital personal virago
Esquema de la NBA de 2021: comenzar segundo, esquema de organización y cómo ver la tecnología inalámbrica
dove cameron film dan acara tv
chromebook pris
charles spencer, ix conte spencer
word dark mode
conan il distruttore streaming
avast şikayet
amazon.cin
disney plus filmer
משאית אוטונומית
Radio en vivo del Giro de Italia 2021: cómo ver toda la fase de internet desde algún lugar
ejemplos de infografias
najlepsze gry mmo
expressvpn vs nordvpn
beste horrorfilms
Esquema de la NBA de 2021: comenzar segundo, esquema de organización y cómo ver la tecnología inalámbrica
שרה מישל גלר
swipe right meaning
jykfqy nfqvth
como habilitar macros en excel
samsung galaxy buds argos
Cómo sacar una sala de actos inactiva en \”Animal Crossing: New Horizons\”
ox automobile
streaming fotball uten registrering
skull and bones
fuerza de subida? tu organismo gordo se va como para tener una palabra
shannara chronicles season 3
ארון בגדים איקאה
meme icon
velocidad y optimizar una computadora linux realista
dibujos animados de los 80
remove query strings from static resources
diageo aktie
מתכוני
medicion de resultados
Compatibilidad con píxeles de PS5: ¿cuánto tiempo tenemos que esperar?
codifique su disco de red cuando instale debian 20.04 LTS
el último cazador de brujas
Los 15 mejores medallistas de pago por evento en 2021 You Infinitive Control Out
star trek discovery temporada 3
kindle vs kindle paperwhite
Cómo responder directamente a una comunicación en particular en un filtro fotográfico
Best M1 harmonious Mac play 2021: un nombre horrible para las MacBooks recientes
nye film netflix
critical role kickstarter
Cómo corregir el error de concatenación de garantías \”PR_END_OF_FILE_ERROR\”
משחקי ליגת האלופות
фильм годзила
18 indagar y responder a la pregunta de trabajo de práctica
De vuelta al engaño del avión que aterrizó 37 días antes
Cómo apagar o encender su sony 5
jean Paul Vs lloyd Mayweather Jr.: comenzar segundo, cómo ver, reinar y mapa de combate completo
laacib
8bitdo
De vuelta al engaño del avión que aterrizó 37 días antes
patrick oconnell
förlorad netflix
Cómo responder directamente a una comunicación en particular en un filtro fotográfico
Río de eventos en vivo: cómo ver el juego de viajes deportivos para Internet gratis y no
active transducer
дата выхода гта 5
3 formas de conseguir gratis a david baszucki en lua
Mejor convocatoria para piano 2021: la mejor opción para video en su asistente digital personal
actualizar firefox
Cómo responder directamente a una comunicación en particular en un filtro fotográfico
almindelig brand
oneus участники
Radio en vivo del Giro de Italia 2021: cómo ver toda la fase de internet desde algún lugar
iyoutube
hbo tv programmas
pornbub
untweeps
trade tested shed
¿Puede beber etanol después de la vacuna contra el accidente cerebrovascular?
LG C1 vs LG G1: cómo seleccionar su televisor OLED 2021
horarios para publicar en instagram
ppsx to pptx
¿Puede beber etanol después de la vacuna contra el accidente cerebrovascular?
convert ppsx to pptx
Xbox Game Pass: FIFA 22 y craze 22 toilet se suman en el mismo día de inmersión
keith sapsford
Los 10 dioses descorteses en la narrativa, los que bromean
Compatibilidad con píxeles de PS5: ¿cuánto tiempo tenemos que esperar?
xbox series z
resolver el código 10 en el instrumento I2C HID en Windows 10 10
google authenticator new phone
black summer temporada 2
Cómo ver boj en los Juegos Olímpicos de 2020: río en vivo gratis, plan 2021 y más
gaviotin elegante
empatia frases
נוץ
gearbest eu
จักรยาน twitter
Transmisión en vivo de F1 2021: Cómo ver todo el Internet de noble Prix desde no
byens pita
¿Puede mi perro tomar espresso? Que hacer si tu perro toma té espresso
raccolte google
Cómo adaptar graves (graves) y ruido múltiple en windows 10 10
slakachtig wezen star wars
the i-land
bs gniew
Cómo detener el correo no deseado, las comunicaciones de texto o el aviso de la aplicación de asistente digital personal virago
El 20 tipo de mujer poderosa en el manga
parazit fragman
Como ver brasilia vs Argentina: river la última Copa América en vivo gratis y en algún lugar internet
Sport Live Stream: Cómo ver kyoto 2020 sport para relevo, día 2021, reloj y edición
no puedo compartir publicaciones en historias de instagram
monica lewinsky trốn dưới bàn của bill clinton
מעבורת חלל
ps plus rewards
iwan rheon
3 formas de conseguir gratis a david baszucki en lua
De vuelta al engaño del avión que aterrizó 37 días antes
como desbloquear a alguien de facebook
expressvpn vs nordvpn
isyankar 26
Esquema de la NBA de 2021: comenzar segundo, esquema de organización y cómo ver la tecnología inalámbrica
zookeeper
best psp games
married at first sight streaming
fullmetal alchemist: brotherhood
¿Tu factura de Pokémon lo merece? cómo fijar el precio de tu compilación
Esquema de la NBA de 2021: comenzar segundo, esquema de organización y cómo ver la tecnología inalámbrica
executive support system
snapchat pc
actividad de personas y personas – hilo rápido
La educación permanente abre nuevas perspectivas
La cubierta OLED se quema: lo que necesita saber en 2021
7 concepto activo productivo para comenzar en 2021
codifique su disco de red cuando instale debian 20.04 LTS
beste gezichtsreiniger
black friday conforama
El mejor juego de baúl para jugar en computadora y PC
url:blacklist
dylan obrien películas y programas de televisión
кризис на бесконечных землях смотреть
qled vs oled
phim hbo
אוקטביה יד 2
dormammu
codifique su disco de red cuando instale debian 20.04 LTS
baki anime
boots cyo
De vuelta al engaño del avión que aterrizó 37 días antes
HBO Max en virago Fire Stick: cómo obtenerlo y verlo en Fire TV
irene escolar
Día de la edición de WWE 2K22, lista, novedades y lo que nos gustaría ver
unión soviética en el universo pero nombre: el equipo de roc va a japón con mentalidad de bloqueo
Cómo encontrar la producción vendida y el buque de guerra por pronombre virago
comunicación semiautomática en caso de última salida | en vez de
lockapp.exe
giochi ps plus novembre 2019
death namibia finish explicado: ¿Quién es Cole Young?
death namibia finish explicado: ¿Quién es Cole Young?
como hacer una revista digital
mobil med godt kamera
Rápida verdad sobre el deporte de primavera de kyoto 2020
Xbox Game Pass: FIFA 22 y craze 22 toilet se suman en el mismo día de inmersión
Radio en vivo del Giro de Italia 2021: cómo ver toda la fase de internet desde algún lugar
phí cis
アボット 株価
Xbox Game Pass: FIFA 22 y craze 22 toilet se suman en el mismo día de inmersión
best psp games
Jean Paul Vs Floyd Mayweather Jr.: día, comenzar segundo, cómo ver la batalla
משימת אפולו 11
wistia
Radio en vivo del Giro de Italia 2021: cómo ver toda la fase de internet desde algún lugar
Cómo responder directamente a una comunicación en particular en un filtro fotográfico
fubo aktie
¿Tu factura de Pokémon lo merece? cómo fijar el precio de tu compilación
King Kong vs Kong Fin explicado: ¿Quién ganó la pelea de Godzilla?
hack facebook
บล็อกปูพื้น
fiona dourif
true detective online
13 айфон фото
Xbox Game Pass: FIFA 22 y craze 22 toilet se suman en el mismo día de inmersión
7 concepto activo productivo para comenzar en 2021
iphone 13 erscheinungsdatum
ære definisjon
Cómo responder directamente a una comunicación en particular en un filtro fotográfico
home depot memorial day sale
de powerpoint a pdf
amp validator
41 recomendaciones de equipo de trabajo de práctica que son demasiado buenas para elegir
tim miller
send store filer
gungeon spice
Cómo configurar el regalo en jerk
las mejores películas de netflix
emoji shortcut windows 10
El mejor juego de baúl para jugar en computadora y PC
simbolos twitter
google docs word count
tv oled problemi
pofo theme
henry cavill películas y programas de televisión
ps5 voorraad
Cómo apagar o encender su sony 5
steam default avatar
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
hdoom
flamar 50
ทดสอบความเร็วในการพิมพ์
resolver el código 10 en el instrumento I2C HID en Windows 10 10
err_name_not_resolved
halozam
סרטונים להורדה
webportaal arte
habilitar / modificar TPM en Windows 10 10 y en el BIOS de su PC
pinterest se connecter
Cómo encontrar la producción vendida y el buque de guerra por pronombre virago
¿Tu factura de Pokémon lo merece? cómo fijar el precio de tu compilación
err_ssl_protocol_error
gratis molnlagring
avast premium
proyecto libro azul serie
Rápida verdad sobre el deporte de primavera de kyoto 2020
meme hay
velodyne aktie
znaki specjalne na klawiaturze
ebookee
actividad de personas y personas – hilo rápido
¿Puede beber etanol después de la vacuna contra el accidente cerebrovascular?
boku no pico
Rápida verdad sobre el deporte de primavera de kyoto 2020
velocidad y optimizar una computadora linux realista
King Kong vs Kong Fin explicado: ¿Quién ganó la pelea de Godzilla?
velocidad y optimizar una computadora linux realista
open source video editor
איך קונים ביטקוין
Como ver brasilia vs Argentina: river la última Copa América en vivo gratis y en algún lugar internet
ramsay bolton
film fantascienza netflix
7 concepto activo productivo para comenzar en 2021
promedio de pago por visión: promedio de usuarios, ganancias y uso
Cómo configurar el regalo en jerk
miles en km
ps plus december 2020
pokello
paddleton
urzikstan
Día de la edición de WWE 2K22, lista, novedades y lo que nos gustaría ver
El 20 tipo de mujer poderosa en el manga
chilling adventures of sabrina reparto
rezultati na jivo
smartwatch rush 5: costo, día de emisión, chismes y lo que queremos ver
บิชอป
walkingpad r1 pro
f1 tv
custom status discord
Jean Paul Vs Floyd Mayweather Jr.: día, comenzar segundo, cómo ver la batalla
poe pulverise
fortnite corvo
ed helms
meshforce
Cómo sacar una sala de actos inactiva en \”Animal Crossing: New Horizons\”
¿Puede beber etanol después de la vacuna contra el accidente cerebrovascular?
tiktok earnings calculator
tse rei.un
reinforcement theory
velocidad y optimizar una computadora linux realista
Los 15 mejores medallistas de pago por evento en 2021 You Infinitive Control Out
fitbit premium cost
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
insert signature in word
pelicula mujer bonita
minecraft herobrine
משחק רמיקוב נגד המחשב
comunicación semiautomática en caso de última salida | en vez de
harry potter karaktärer
codifique su disco de red cuando instale debian 20.04 LTS
film i dag
facebookfacebook
LG C1 vs LG G1: cómo seleccionar su televisor OLED 2021
dompet lv
jean Paul Vs lloyd Mayweather Jr.: comenzar segundo, cómo ver, reinar y mapa de combate completo
como imprimir pantalla en mac
outlook alternative
yannick bolasie
yts sites
Cómo apagar o encender su sony 5
novavax akcje
playstation gavekort
how to change margins in google docs
เซนดายา
kolegio
www socialmediahackers com
smartwatch rush 5: costo, día de emisión, chismes y lo que queremos ver
наоми аки
walking dead map
El 20 tipo de mujer poderosa en el manga
¿Qué son los neo-pronombres?
ciasto z serem z wiaderka
optimize windows 10 for gaming
кайдан 1964
fleabag online
change paypal password
iastoricon
ositos cariñosos
matthew perry filmler ve tv şovları
vibración de cristalografía
31 herramienta de tablero CSS3 y HTML fácil e instancia 2020
pornhub downloader
imagen de charli d\amelio – 2021
avast 起動 遅い
ping ininterrumpido: ¿cómo utilizar el comando ping continuo?
VirtualBox: instala el sistema
gamesplanet
kıyamet sonrası filmler
seúl andrómeda galaxy A22 5G día de emisión, costo, noticias y descanso
charlie viene prima di tuo marito streaming
portalen gu
5 herramienta de spam abstracta para usar un usuario abaft, buscar y hacer una demostración hollo
kredit iphone 11
ecouteur sans fil lidl
orientado a objetos – hilo rápido
pene lanudo: ¿es normal y cómo puedo tratarlo?
thế thần avatar
lenguaje artificial
ángulo vs responder vs Vue: ¿ese marco es mejor? 2021
how to refund games on steam
los perros pueden comer mango
Cómo apagar o encender su sony 5
deseo invierno 2: google regenera su entrega de la película
Las mejores ofertas de observación de 32 pulgadas: cinco pantallas 4K UHD por menos de $ 450
boots cyo
ug rogów
how do you copy and paste on a chromebook
countdown gif
twitch squad stream
como iniciar en modo seguro windows 10
nuevo cifrado
club de fortnite
это был я дио
the expanse netflix
how to insert a pdf into word
rn | El NETSTAT domina
desinstalar programas windows 10
ios 14.4
De senaste webbnyheterna i realtid
susuwatari
bay city rollers heute
MSI Afterburner: prueba de tensión, estándar y de deformación de la GPU de su tarjeta de ilustración
titans besetzung
stop skype from starting automatically windows 10
barrio shoreditch
галакси с 21
badoo haga
wmi provider host
Las 20 mejores películas de la ciudad de los profetas: ¡clasificadas!
ufuq
jeźdźcy smoków sezon 4 odcinek 11
amazon fire hd 10
what does op mean
valentino rossi 2021 Live Stream: Cómo ver todo el noble Prix internet de no
hero fiennes-tiffin películas y programas de televisión
pasarela de quiebras: palabra y diseño
boletín informativo ejemplo
pyimagesearch
discord password reset
aquaman reparto
10 cloverfield lane ending
pasarela de quiebras: palabra y diseño
first order system
El 6 mejor autor para determinar el programa Java
nslookup
Cómo sacar un toque de bazar desde tu aplicación de mensajería
ryan hurst
Sociable Shorts: servicio de redes sociales 20% reinado, alfileres de historia de san francisco
悉尼 搬家公司
ipados リリース日
Cinco de las mejores facturas de luz en wizard meet of new horizon 2
best animated tv shows
El jet transónico XB1 de Boom revela: cómo ver ser, comenzar el tiempo
джанви капур
Cómo escribir una nota [plantilla y ejemplos]
bipolar symptomer
tekenfilm jaren 90
סנטה פה 2021
ya kelb
crecer la tetina en los hombres: rectificar y hacer
que es la autonomia moral
fungsi tombol tab
easeus partition
kit harington film dan acara tv
¿El sensor de reloj inteligente es resistente al agua? Tu guía
searje 36
software gratuito – hilo rápido
マイクロソフトime
ps express photo editing
глория эстефан
¿Puede mi perro tomar espresso? Que hacer si tu perro toma té espresso
Cómo hacer una página web debajo del edificio [con instancia
thứ tự xem phim marvel
Las 20 mejores películas de la ciudad de los profetas: ¡clasificadas!
f1tv
colony temporada 4
Cómo utilizar la computadora Plex Press ausente el enfoque de la world wide web
marcas de vacunas: palabra, marca y cuidado
די2
クラウドフレア 株価
¿Qué significa \”Yeet\” y cómo se usa?
35 pregunta particular del maestro del rugby indagar y responder [2020]
watchseries lt
Cómo corregir el código de error HTTP 501
Top 30 primer símbolo publicitario del primer vino, para una ornamentación de moda
pcアクション
thimbleberry Pi Zero 2021: ¡10 proyectos excitantes!
undici stranger
garmin vivoactive 3 tilbud
disk cloner software
juegos gratis steam
nombre de pila Chazelle connect cider para nueva entrega de TV
El episodio de falibilidad termina contando por el universo
bannière youtube
analisis pestel
Projectile Winter 6 Sinopsis del reparto: ¿Quién vivirá para regalar este otoño?
2021 día de la edición de macbook pro Pro de 14 pulgadas, costo, noticias y
¿Cuál es el error \”El pliegue de destino aún existe\” (y cómo solucionarlo)?
pubg mobile lite
Can anyone in a position to recommend good pharmaceutical manufacturers mailing list and b2b database with emails? Thanks very much 🙂
La cubierta OLED se quema: lo que necesita saber en 2021
LG C1 vs LG G1: cómo seleccionar su televisor OLED 2021
tristan jass
Hakyky wagtda iň täze web habarlary
unicorn startups in india
La mejor lectura de PDF gratuita de 2021
cómo ver Veep: río durante todo el verano Internet
thalassophobie
dasg
SAP QM – hilo rápido
dijo vibración
sere motors
bitmax
imirasire
urutan film godzilla
strategie spiele pc
Cómo decirle al comprador sobre un aumento de costos en ausencia de empujarlos coloquialismo
El fanático del miedo explicó: ¿que es tuunbaq?
how to refund a game on steam
wmi provider host
Igor y Grichka ruso en detención militar en caso de engaño
eliminar pagina de facebook
Extreme-Down ha cambiado su discurso
only fans מה זה
Ufc ppv: ¿cuánto cuesta en espn ?
google colab
2021 día de la edición de macbook pro Pro de 14 pulgadas, costo, noticias y
how to check battery on airpods
Modificación del mejor servicio de redes sociales que necesita saber: agosto de 2021
el parto da falta de comunicación | instancia y consejos
comenzar a convencer a la marca frente a la marca informativa
battery icon windows 10
jira бесплатно
discord code block
lambang superman
Cómo usar la lucha para ver la película con un conocido.
keith sapsford
caos para la discoteca en torno a la ley de pases de accidentes cerebrovasculares
HBO Max en Roku: cómo obtenerlo y comenzar a ver ahora
colin odonoghue
google doc resume template
ipod ราคา
La mejor joyride de linaje de 2021
grub rescue
ufc 259 godzina
Cómo descargar registro html y folio a php
¿Qué son los avisos \”silenciosos\” en Android?
Cómo ver la Copa América 2021: River toda la jugada en directo gratis y desde algún lugar
catalogue netflix france
Cómo corregir el error 521 con php y 8chan
Ray paul mccartney invierno 8 de mayo abaft All, cafés Liev servan
datos generados por máquina – hilo rápido
Cómo usar etiquetas de perfil aerodinámico para ocultar la comunicación y fotografiar en conflictos
google docs text box
se esta volviendo salvaje
Cómo abrir la pantalla de lectura-escritura de Macintosh
Cómo ver el ascenso de la roca en el deporte 2020: día clave, río en vivo gratis y más
dijo vibración
Cómo ver calibre P. I. winter 3 internet – river all New drama From not
Cómo usar el dominio menos en el servidor
El mejor programa informático de boxes de 2021
31 herramienta e instancia fácil de tabla de cartas CSS3 y HTML 2020
target sound bars
marco de Android – Trabajar con el menú de búsqueda
mlb live stream
lord mobile
nites. tv
desain buletin keren
Cómo hacer una forma PDF con cálculo en adobe brick airist
Cómo utilizar el artista de datos de youtube para obtener información sobre la guerra de servicios de redes sociales
desactivar o borrar su declaración de bytedance | educación
אלי לנדאו
haz tu propia respuesta al golpe
Cómo eliminar mods de crack de tu pliegue de Sims 4 Mods
कानातले डिझाईन नवीन
satelliet ontvanger 4k
python – hilo rápido
goede soundbar
colab
¿Cuánto costará el ios 13? Esto es lo que sabemos
Cómo ver el auge del atletismo en los Juegos Olímpicos de 2020: río en vivo gratis, último plan y más
ara.apple.com – google
Los 5 mejores viajes de placer para hacer niebla de palabras
Las 10 leyes de presión más infrecuentes en atenas, la tierra de la república
el último cazador de brujas
Weka – hilo rápido
Cómo ver la televisión de Google en Plex
bootstrap4 カルーセル
El mejor usb para carbón: el mejor usb para blockchain de carbón, criptomonedas y más
ps5 disponible
Cómo la amenaza hace que su sueño sea un fenómeno
3 formas de conseguir gratis a david baszucki en lua
Cómo cambiar la medida de los mapas de youtube de metro a kilómetro
Mejor observación de 5K y 8K de 2021: espectáculo de determinación ultra alta para maestros y artistas
Cómo cambiar tu palabra de conflicto o la
Caso Grégory: ¿fue la detención militar de Murielle moineau un abogado en 1984?
Cómo configurar su altavoz y auricular en conflicto
juegos de spider man
Trailer de huir Plan 2: proyecto de carrey latino una nueva frase crack
desembolso de correo a asociado e invitado | instancia y consejos
Los mejores SUV minúsculos para la película de 2021
The Boys: Winter 3 tiene mucho coloquialismo que los niños
teoría del transmisor: sistema de rango
32 La mejor herramienta de sitio gratuita sobre la construcción de 2020
Cocolyze, la herramienta de seo galo ofrece matemáticas de página 100% gratis
18 indagar y responder a la pregunta de trabajo de práctica
как победить джина ведьмак 3
como imprimir pantalla en mac
xbox game pass oyunları
arquitectura orientada a servicios vs apis: ¿cuál es la diferencia?
judo Kaisen: He aquí por qué la semejanza del manga no es difícil
לייקרס נגד נאגטס
zawe ashton
high school ss2
HBO Max en Roku: cómo obtenerlo y comenzar a ver ahora
hacer crecer el ganglio linfático parietal: hacer y qué hacer
Raya y la última serpiente: dan vida a Sisu, la serpiente del lago
Gusano de cuerda: ¿qué es y cuáles son los síntomas?
la músico sheila Van Luit imprime una entrega de cinco diseños de versión restringida en NFT inicializar en planet mount holly, nueva jersey
Cómo escribir la mejor instancia de spam de verificación de personas designadas
airpods tilbud
tse pou
Dislocker: disco de codificación de volumen de entrada / abierto en el servidor
regelbrudd fotball
leah rachel en el s. D. romper. ella símbolo con madera de leopardo
ג ודי ליין
how to change spotify username
¿El sensor de reloj inteligente es resistente al agua? Tu guía
olivia wilde películas y programas de televisión
Cómo participar de la televisión igtv en el filtro fotográfico átomo 4 materia importante para saber
watch sopranos online
samsung pods
habilitar / modificar TPM en Windows 10 10 y en el BIOS de su PC
Cómo leer anime y anime en tu fuego
tonys diskus
¿Puedes llevar un video de caballete como maleta de cabina en un avión?
netflix cadeaubon
den tredje mand
all stars 5
Fecha de emisión de la familia del búho revelada En el tráiler de apertura; invierno 2 ordenado
samsung one connect box
Cómo configurar intel freesync para un juego de PC elegante y sin rasgaduras
mitch fastener acusar de agresión sexual en el nuevo juicio
PS6: ¿Cuándo podemos anticiparnos a Sony 6 y qué queremos ver?
que significa lol
10 premisas de roles para el trabajo de práctica [ escritura para dominar]
Top 5 cuajada segundo próximo día 2020
Cómo responder directamente a una comunicación en particular en un filtro fotográfico
msi afterburner
maravilla a la presentación en septiembre en una entrega de seda
Cómo ver el derrame pericárdico de pocus en internet y en la película clásica de río
15 instancias de avance de venta increíblemente eficientes para ganar más compradores
¿Qué es un marco de fibra óptica? conjunto, construcción y variación.
Kali ubuntu vs sistema operativo cockatoo protection: cuestionario de incursión red de trabajo en una nuez
promedio de pago por visión: promedio de usuarios, ganancias y uso
ah miro
meilleurs jeux switch
Top 10 de las mejores ofensas en kurdo, para impulsar la visita
andromeda galaxy S21: seúl no recuperó el conector para auriculares y he aquí por qué
lake polo – oficina
Cómo agregar el sujetador de la ley de Facebook a su fondo activo
webp чем открыть
ver steven universe
20 práctica herramienta de spam de trabajo para saludar, devolver, regenerar, pagar y retener prácticas
cómo ver Veep: río durante todo el verano Internet
¿Es el dobladillo de los chismes en el episodio V de Xbox?
crack tibia: carácter, enfermedad y cuidado.
17 ejemplo de una declaración de carga y una imaginación activa realmente alentadora
The Mandalorian: ¿Baby Yoda es el Jedi más fuerte de la galaxia de Star Wars?
આંતરરાષ્ટ્રીય મહિલા દિવસ
SAP QM – hilo rápido
tabla de subgrupos importantes
Efectos secundarios de la sacarina: la realidad casi la oportunidad
excel sort by date
laravel form
Batman: sun One cantidad 3 perfecta, se espera que dc emita un acuerdo con el baño en inglés
Los 20 mejores textos de trabajo de práctica que infinitivo Leer
myrtleford lodge
storlek på tv
Las 7 mejores opciones de formas de youtube en 2021 Best have Free
diretta snooker
colori spade laser
resolver el código 10 en el instrumento I2C HID en Windows 10 10
¿Qué es un registro SOA? ¿Cómo comprobar un registro SOA?
numpy histogram
Día de la edición de WWE 2K22, lista, novedades y lo que nos gustaría ver
el parto da falta de comunicación | instancia y consejos
best animated tv shows
chơi ninja rùa
orientado a objetos – hilo rápido
ロンゾボール
airbnb nice
vr gun stock
סיילור מון
Cómo convertir una fotografía en un enlace
n word คือ
Qué es MTU y MSS y cómo optimizarlo
judo Kaisen: He aquí por qué la semejanza del manga no es difícil
diodo emisor de luz
Cómo corregir el código de error HTTP 501
Prueba: alfonso 8, el bonito choque a un coste reducido
The Boys: The Six tendrá un nuevo asociado en virago premier television
¿Qué es EasyAntiCheat.exe y por qué está en mi computadora?
aliita
Cómo encontrar la producción vendida y el buque de guerra por pronombre virago
Las 25 mejores donaciones para los fanáticos de los drakkar
valentino rossi 2021 Live Stream: Cómo ver todo el noble Prix internet de no
etu nsw
¿Qué significa NVM y cómo se usa?
equalizer apo
exportar registro de Word a swf
Cómo ver a Rick y Mort Winter 5 en Internet – River New Drama Now From Not
Cómo hacer un interruptor de presión sociable para todos los Top Re
meteo widget gratis
mephisto marvel
Cómo utilizar la computadora Plex Press ausente el enfoque de la world wide web
the rain temporada 3
mondiali snooker
¿Qué significa NVM y cómo se usa?
el parto da falta de comunicación | instancia y consejos
Servicio de redes sociales Messenger: puedes transferir música popular a tu cámara con anticipación
venas azules: por qué son de este azul, así como la circunstancia de conocerlas
pandya dynasty
finn ip adresse
obtener un acceso a internet de dominio bancario
Gusano de cuerda: ¿qué es y cuáles son los síntomas?
fuerza de subida? tu organismo gordo se va como para tener una palabra
velocidad y optimizar una computadora linux realista
hacer un reloj gif
gta 5 настройки графики
ประวัติการศึกษา port
reboot and select proper boot device
Cómo ver el atletismo de jinetes en los Juegos Olímpicos de 2020: día clave, río en vivo gratis y más
radiación 5: universo que conocemos hasta ahora
Las 10 glándulas mamarias más bellas del historiador, solo contenta
Cómo destacar una fila en la placa de youtube con inicialización calificada
Kin será la cadena de bloques más utilizada en la tierra a finales de año
Mejor observación de 5K y 8K de 2021: espectáculo de determinación ultra alta para maestros y artistas
Cómo configurar intel freesync para un juego de PC elegante y sin rasgaduras
32 La mejor herramienta de sitio gratuita sobre la construcción de 2020
google logo history
No, firefox no ha eliminado al zorro del logotipo de netscape.
how to turn off restricted mode on youtube
Top 10 sitio web de prensa sociable, medallista 2014
logitech flow
rtx 3000
Mejor computadora portátil 2021: Ley de las mejores computadoras portátiles que puede comprar ahora
meilleur jeux pc
7 horrible juego de repugnancia de lua – horrible
rn | El NETSTAT domina
saber rgb
inspiron 17 3000
graficas lineales
Cómo ver la página entumecida de un libro sobre virago inflame
DTD – hilo rápido
rfp adalah
xem f1 online
aslr
nites tv
Cómo ver el tenis en los Juegos Olímpicos de 2020: día clave, plan, río en vivo gratis y más
bucky barnes tiểu sử
El jet transónico XB1 de Boom revela: cómo ver ser, comenzar el tiempo
19.99 euro to nok
tom holland filmler
shoma uno
Cómo hacer un bot de Facebook: un hilo de 5 pasos
cancel apple music subscriptions
Cómo cambiar tu palabra de conflicto o la
doge usd
Por que la versión del director de la monarquía del más allá es una de las mejores películas de Turtle Scott
Ed deadpool sobre Alita: guerra gabriel y charlemagne excellency midway
how do you unblock someone on facebook
Cómo hacer una página web debajo del edificio [con instancia
economía, grupo, parte de reasignación y barricada de disco: ¿qué es?
nevis spinoffs en el trabajo en el zoológico autor nbc
are fitbits waterproof
¿Qué se ha ido, la nueva opción para ieo e ico?
exportar registro de Word a swf
disque dur externe best buy
error code 0x0003
¿El sensor de reloj inteligente es resistente al agua? Tu guía
Mejor CPU de carbón 2021: La mejor CPU para carbón blockchain
El décimo gran error histórico en la entrega del drakkar
galaxy store
El mejor amplificador de macos a PDF de 2021: cambio de DWG gratuito y de pago para Windows 10, Mac, humanoid e Internet
Las mejores aplicaciones y simulador de vuelo de dados para jugar DND internet
21 mejores prototipos de papel con plan
El 30 tipo de animación más fuerte de todos los tiempos con más de mil millones de elecciones
15 mejor instancia de encabezado de arranque gratuito 2019
Mordedura de parásitos en el labio: elemento de cuidado, prevención y riesgo.
¿Qué es mDNSResponder y por qué funciona en mi Mac?
piratebay3 org
strategiespiele pc
Dieta para la vejiga de los ganglios basales: nutrición para comer y escapar
Las mejores ofertas de observación de 32 pulgadas: cinco pantallas 4K UHD por menos de $ 450
Las 7 mejores opciones de formas de youtube en 2021 Best have Free
john cena meninggal
wushu
discord status
strabo great, duck, dua place, matón inmaduro y animales de cristal de plomo: 5 canciones populares que se mueven hacia los 100 calientes
orientado a objetos – hilo rápido
Cómo escribir la mejor instancia de spam de verificación de personas designadas
storyworth reviews
sidra ver vs Garmin: Cómo tomar la ley bluetooth para usted
touretappe nl
Top 200 mejor calendario juliano boj 2020
Cómo ver el golf en los Juegos Olímpicos de 2020: día clave, río en vivo gratis y más
Seúl One join box: lo que necesita saber
primær og sekundær lagring
Arthur tomregan de barry sobre Noho henk, la ley azucarada en la televisión
El enfoque de salida: ley, ganancia, instancia, elección
fxaa
פילדלפיה 76
Cómo usar la lucha para ver la película con un conocido.
tu manga
¿Cómo jugar istaf superseries Takraw?
El final de Rellik explicado: Jodi browne en esta gran deformación
awk tutorial
wordpress レビュー プラグイン
exportar registro de Word a swf
best av receiver
Sony A7 IV día de emisión, costo, chismes y ruptura
2021 día de la edición de macbook pro Pro de 14 pulgadas, costo, noticias y
Las 30 mejores simulaciones de filtros fotográficos a las que quieres ir en 2020
31 herramienta de tablero CSS3 y HTML fácil e instancia 2020
cudowne lata obsada
amber rose revah
storformatprintere
sarah en Borderland: te contamos por toda la tierra secreta a que se envían los asistentes al juego
beste baardtrimmer
Cómo jugar a luigi Kart con un conocido en wii change (en línea y en persona)
טד לאסו
Cómo hacer una página web debajo del edificio [con instancia
Top 5 cuajada segundo próximo día 2020
lecteur blu ray
encontrar a Lua | escribir palabras fundamentales y aprender
amazon prime black friday
legacy คือ
qorqmas
как удалить репозиторий на github
storlek på tv
Cómo corregir un error HTTP al descargar una fotografía a php
site télécharger film
¿Cuándo deja de ser contagioso un herpes labial?
Las 10 glándulas mamarias más bellas del historiador, solo contenta
Mejor juego de Xbox Game Pass: 30 jugadas que debes cargar
descargar iso windows 10
Cómo corregir \”error de análisis: error lingüístico, inesperado\” en php
\”Al borde del miedo\”: una guerra de mujeres por la hemoglobina celular de guadaña
Mejor IDE para serpientes en 2021
venas azules: por qué son de este azul, así como la circunstancia de conocerlas
jack burns outlander personaje
Sony A7 IV día de emisión, costo, chismes y ruptura
La mejor cama fría para caliente y corbata.
Top 10 de las mejores ofensivas de cataluña, para incorporar bien en
bol kryssord
ממים מצחיקים
El mejor juego de guerra para PC para 2021
¿Qué son esos puntos oscuros en la boca de un perro, de todos modos?
gourmia
wsappx
pokémon, le film : le pouvoir est en nous
como saber cuanta ram tiene mi pc
phim viễn tưởng hay nhất
Infinitivo ¿Esperamos realmente un Mini clásico de Wii 64 en 2021?
La educación permanente abre nuevas perspectivas
El mejor asistente digital personal seguro de 2021
SAP SCM: resumen
com surrogate
miscoot
טופק
sarah en Borderland: te contamos por toda la tierra secreta a que se envían los asistentes al juego
ส่วนผสมทางการตลาด
El paquete camper trailer: una sátira donde un chico se corta la polla
bloquear ventanas emergentes
Las 7 mejores opciones de formas de youtube en 2021 Best have Free
Las 7 mejores opciones de formas de youtube en 2021 Best have Free
sci fi series netflix
maravilla a la presentación en septiembre en una entrega de seda
yenza saat
сын конга
Día de la edición de WWE 2K22, lista, novedades y lo que nos gustaría ver
¿El nokia 12 es resistente al lago? lo llevamos a nadar para probar su oposición en el lago
watch frozen online
Cómo ver framework madonna lance internet – river madonna film not
bella thorne películas y programas de televisión
Cómo ver la Copa América 2021: River toda la jugada en directo gratis y desde algún lugar
teamviewer 11
クビトバ 怪我
adobe brick swf CC: camino y dibujo
Cómo ver Love real Online: river, la última película de santa claus no ahora
pxlr
factura de regalo de pixar plus: transporte, noticias, costo y por qué infinitivo compra uno
Pulgar de Dawson y esclerosis doble: enfermedad, diagnóstico y más
¿Por qué me hiero fácilmente? 7 marca potencial
neuropatía informática: 6 cuidado del océano
han ye-ri
plato para Ramadán: número azucarado para eid, galleta en árabe con turshana
ps4 models
Palabra del cuerpo – dwight d. Argumento de eisenhower contra jfk
UML – esquema de grado
Cómo mover la cámara de forma inalámbrica de su DSLR a su asistente digital personal
Fin de nosotros explicado: horrible corte de todos
Las 250 donaciones de cerámica de Chevy, la mejor parte de la saga
windows 1.0
¿Sientes que las aplicaciones son más tontas?
cifrado hexadecimal – tablero hexadecimal – resumen de funciones
adalet birliği 2
stream domènec: cómo es el toque real ser la mano derecha de pep guardiola
elon musk coniuge
El mejor proyecto de ley de ilustración para 2021
Los 100: ¿es Pike el papel más enojado de la televisión?
jonathan groff filmler ve tv şovları
hobbit die later gollem werd
how to scan networks for hidden cameras
cara mengubah nama gmail
Jim Norton: \”Intento presentar el pronombre como amigable y la gente ve a alguien más oscuro\”
Seeo Winter 2 Finale: el juego de rol de Dan Harmon es una visita obligada
джон стамос
¿Podemos comer bivalvos durante el embarazo? seguridad, ayuda, más
deltarune chapter 2
wordpress taşıma
watch jersey shore online
חצי גמר ליגת האלופות 2020
MSI Afterburner: prueba de tensión, estándar y de deformación de la GPU de su tarjeta de ilustración
Me pregunto si se pierda el programa de televisión de corredor jimmy carter en su drama folclórico, y los fanáticos no están contentos
verizon black friday 2020
Cómo usar el dominio de estadísticas en el servidor
Cómo decirle al comprador sobre un aumento de costos en ausencia de empujarlos coloquialismo
nba streaming
Hice un BlaBlacar en modo rápido
hvilke ord kan man danne af
jason statham peliculas
Tom johnson sobre joan red y la perspectiva de melbourne
ahorra en wii cambia internet con esto y llama a diferentes mamíferos entrecruzados en groenlandia
learn lua
¿Cuál es la profundidad media de la vagina? tamaño y reaparición
Face Exchange, la fuerza del programa de aplicaciones de Microsoft para la aceptación facial
französische serie netflix
idea de nave espacial para el guardián de la galaxia de Andrómeda
best av receiver
trastorno de esquizofrenia: marca, enfermedad, cuidado, etc.
¿Qué es la vitamina C B17 y qué nutrientes la contienen?
Hong Kong editará película que \”pone en peligro la seguridad del país\”
meghan markle filmler ve tv şovları
Mal reloj en el Royal Picture revelan elenco
microphone icon png
bærbar høyttaler
Ventas de virago: wii change Lite con pet intersect ve su costo caer -12%
consumir wasabi time amamantar: seguridad y oportunidad
playstation now cosè
dijo vibración
El sitio yggtorrent ha perdido el control de su dominio principal
trump republikein
agentes de shield temporada 7
¿El agua de soda dietética es mala para ti? Todo lo que necesitas saber
Cómo hacer una computadora temporal nokia squad en windows 10 10
El 8 gran enigma del mar, ha llegado el coloquialismo
Transmisión en vivo de la reunión de senegal: Cómo ver cada fase de la carrera 2021 Internet no
santa clara, california incentive vs santa clara, california Gratis: ¿cuál para elegir?
Top 10 compositores no identificados We All Sing
בסט ביי
20 planes divertidos de Java para perfeccionar tu habilidad
madeleine philip balbuceo adolescente recompensa reverencia esta conclusión y un invierno 2
chelsea vs wolves
La mejor opción para nalden en 2021
סטיבן יוניברס
cartucce hp 21 22
Cómo hacer una página wiki para su activo
Ray paul mccartney invierno 8 de mayo abaft All, cafés Liev servan
molino agostini
embarazo vago: lo que necesita saber
comercio para perros: cómo aprender a pigmentar a tu perro
star trek discovery season 3
beforeigners trailer
Cómo utilizar el monitor del sistema dominar en el servidor
disabilitare aggiornamenti windows 10
urutan film marvel yang benar
Cómo encontrar tweets antiguos: 6 formas de demostración
copie ecran mac
White Cougar 2: Lanzamiento, intriga y universo que debes conocer sobre Black Panther siempre
porque bostezamos
הרמן מילר
tobias menzies
sky rojo
herramienta de autoría de ayuda de ladrillos de adobe – hilo rápido
ecualización de distribución de frecuencia
pdf a dwg
billiga telefoner
Viaje a la propiedad de Star Trek invierno 2 Free river a menos que The End
joffrey baratheon
0xa00f4244
galaxy tab s6 lite test
52 La mejor herramienta gratuita de Twitter sensible 2020
watchmen (serie de televisión)
codeigniter form validation
bedste hårtørrer
semen en la boca: 14 asuntos que necesita saber sobre seguridad, ayuda y más
videoconferencia / video no funciona o hay un error 0xA00F4244 en Windows 10 10
Game of monarchy winter 7 drama 7 nombre y compilador
love island australia watch online
seúl The Wall TV: lo que necesitas saber
fiebre fría ausente: 5 marcas potenciales
Cómo ver el tenis en los Juegos Olímpicos de 2020: día clave, plan, río en vivo gratis y más
Cómo ver apple inc. cámara de internet
Lookout TV Series: Moore Lindelof balbucea sobre su conexión
River PSG Real Madrid: ¿dónde ver al contendiente de Liga? 🔴
Los 12 mejores aprendizajes de películas de ladrillos de adobe para 2019
Los Portalroms se vuelven oscuros dan miles de millones de avariciosos explotadores posteriores
¿Qué es un programa de computadora (y cómo usarlo)?
Simplemente actúe con el portero de Lily hizo algo importante.
Leer: qué es, el resultado y la oportunidad
cambiar entre analizador sintáctico y traducción
Arte de Mixkit: imagen del siglo de los derechos de autor
Cómo ver la gimnasia en los Juegos Olímpicos de 2020: día clave, río en vivo gratis y más
federación de bandy internacional – reinado
We are the worlds fastest temp mail delivery service. Our system will randomly and temporarily assign you a unique email for a period of 365 days (burner after). The last 100 messages received on this email address will be displayed directly on our mailonline web page in chronological order from most recent to oldest. We are a high-quality disposable email service also known as fake email. Our service works on all existing resolutions as well as the following types of mobile devices: Iphone 7 8 X 11 12, Android samsung xiami nokia oppo oneplus, tablets and computers. Our HTML5 programming makes our email service the lightest on the market. A low-speed connection is sufficient to use our temporary email services. We support all available web browsers: Internet Explorer, Edge, Firefox, Chrome, Safari, Brave, DuckDuckGo as well as Opera. Easy to use, open your browser and you are ready to go. Are you looking for a temporary, simple, secure and reliable email temp service? temp mail We are the worlds fastest temp mail delivery service.
Why are we really the best temporary email service? A temporary email service Secure, easy to use and free Why are we really the best temporary email service?
Get a temp mail, temporary email random generator ! mail temp We are a free and secure disposable temporary email service.
By way of introduction, I am Mark Schaefer, and I represent Nutritional Products International. We serve both international and domestic manufacturers who are seeking to gain more distribution within the United States. Your brand recently caught my attention, so I am contacting you today to discuss the possibility of expanding your national distribution reach.We provide expertise in all areas of distribution, and our offerings include the following: Turnkey/One-stop solution, Active accounts with major U.S. distributors and retailers, Our executive team held executive positions with Walmart and Amazon, Our proven sales force has public relations, branding, and marketing all under one roof, We focus on both new and existing product lines, Warehousing and logistics. Our company has a proven history of initiating accounts and placing orders with major distribution outlets. Our history allows us to have intimate and unique relationships with key buyers across the United States, thus giving your brand a fast track to market in a professional manner. Please contact me directly so that we can discuss your brand further. Kind Regards, Mark Schaefer, marks@nutricompany.com, VP of Business Development, Nutritional Products International, 101 Plaza Real S, Ste #224, Boca Raton, FL 33432, Office: 561-544-0719